A. The Law Commission of Ontario
The Law Commission of Ontario (LCO) is Ontario’s leading law reform agency. Our role is to conduct research, undertake public consultations, and develop reports and recommendations to improve the effectiveness, relevance and accessibility of the law. Our work promotes access to justice and contributes to public debate. Over the last 10 years, LCO projects have studied and recommended law reform in areas as diverse as disability rights, consumer protection, and vulnerable workers.
B. What is the Law Commission of Ontario’s Project about?
The Law Commission of Ontario’s (LCO) project, Improving the Last Stages of Life, considers how the law shapes the rights, choices, and quality of life for persons who are dying and those who support them. The project seeks to address the experiences of everyone involved in the dying process, including: individuals, caregivers and other family and friends, health care institutions and professionals, government, other professionals, and community organizations. Our goal is to hear from these groups to better identify and recommend law reforms that are concrete, precise, and responsive to the experience of persons in the last stages of life.
The purpose of LCO’s discussion paper is to encourage and facilitate public engagement on various issues affecting rights and care in the last stages of life and to invite you to participate in our project. In addition to this paper, the LCO will also be organizing consultation meetings, forums, focus groups and individual interviews across the province throughout the spring and summer of 2017.
Ø For a schedule of public consultations and other information about the LCO’s Last Stages of Life Project, please visit our website at http://www.lco-cdo.org/laststages
This discussion paper comes at a critical time. Canadian law, policies and values about death and dying are changing, and there is growing demand for compassionate care that supports a wide range of these values and expectations. Death is an immensely significant experience that each person faces as an individual, family member, friend and participant in broader community networks. Many of us value death and the dying process as a uniquely meaningful stage in life and we approach it with mixed sensibilities – from confusion and grief to a sense of celebration and release.
The “last stages of life” is the broad and inclusive term we use in this project to capture this experience of dying as a process or a continuum of events, whether as a result of terminal illness, chronic conditions or serious frailties that could progress until the end of life. Some such persons may have little time left to live, while others may transition through the dying process for an extended period of years. The LCO’s definition of “last stages of life” is unique. Our objective in selecting this term is to distinguish the experience of persons who are dying – as a particular stage in life – from established models of care that may be beneficial during the dying process, most notably palliative and end-of-life care.
Ø Terms such as “last stages of life”, “care” “palliative care”, “end-of-life care”, “treatment” and “accompaniment” are defined in the Glossary at Appendix A
The importance of these issues cannot be underestimated. The proportion of individuals entering the last stages of life in Ontario is expected to increase appreciably in the coming years as the “baby boom” generation continues to age. [1] Ontarians are also living longer as a result of medical innovations that prolong life; however, we are living longer with chronic illness and complex care needs.[2] Coping with the growing demand for services and supports affects hundreds of thousands of Ontarians; their extended networks of family, friends and caregivers; and countless institutions. Every Ontarian – no matter what their stage of life – has an interest in the dying experience.
The LCO’s project situates these concerns with the last stages of life within Ontario’s legal framework and examines the possibilities for reform. The need for a review of legal frameworks at this time is clear. There are numerous laws and policies that require updating, clarification and simplification, and that currently inhibit access to just outcomes. The LCO’s project asks questions about how to address these challenges, so that the law can facilitate – not hinder – improvements across the health, social and legal sectors.
The LCO has interest and expertise in these issues as Ontario’s leading law reform agency. We provide independent, balanced, and authoritative advice on some of Ontario’s most complex and far-reaching legal policy issues. Our process evaluates laws impartially, transparently and broadly. The LCO’s work is informed by legal analysis; multidisciplinary research; public consultations; social, demographic and economic conditions; and the impact of technology.
As part of this process, the LCO is mindful of rapid and ongoing federal and provincial initiatives actively shaping the legal, regulatory and policy frameworks governing the “last stages of life.” This project has evolved alongside these developments. The key questions asked in this paper have been refined to expand the scope of intersecting issues rather than duplicating governmental initiatives, particularly as they relate to two principal subjects: palliative care and medical assistance in dying (MAID).[8] This paper similarly draws on findings from several completed and ongoing LCO projects, most notably reports regarding capacity and decision-making, older adults, and persons with disabilities. Related ongoing government initiatives and LCO projects are overviewed below, in sections C and D.
Ø For more information on the LCO’s Last States of Life Project Scope Statement, and for regular updates on the project, please visit our website at http://www.lco-cdo.org/en/laststages
Ø To access reports and other documents from the LCO’s past and ongoing projects, please visit our website at http://www.lco-cdo.org/
C. What key questions do these consultations raise?
The paper synthesizes the LCO’s considerable research and background consultations to date, and asks both general and specific questions about key issues. The issues and questions identified in this paper are neither final nor exhaustive. Participants are welcome to make submissions on any additional topics they believe are relevant to the project scope.
Ø A comprehensive list of questions the LCO has posed in this discussion paper is listed in Appendix G, “Questions for Discussion”.
The Importance of Care in the Last Stages of Life (chapter 2): One consequence of the LCO’s inclusive approach to defining care in the last stages of life is that we must account for diversity in Ontario’s communities and regulatory frameworks. The project seeks to address the experiences of everyone involved in the dying process, including: individuals, caregivers and other family and friends, health care institutions and professionals, government, other professionals. It also means considering how the quality of care in the last stages of life varies considerably across different communities of need, which may be defined by age, disability, LGBTQ identity, Indigenous identity, income level, place of residence and homelessness, mental health, faith, culture and others. The LCO has made efforts to explore how diversity influences the issues under consideration in the project. This inclusive approach also means keeping up-to-date with dynamic and ongoing legislative developments affecting the last stages of life.
| 1. | Within the scope of LCO’s project, are there any additional affected individuals, communities, and institutions that should be taken into account? |
| 2. | Are there any additional recent debates or legislative frameworks that LCO should be aware of? |
The Law and Care in the Last Stages of Life (chapter 3): This chapter summarizes existing laws which intersect with the last stages of life. The chapter demonstrates how a wide array of fundamental legal rights and principles affect the delivery of health care. There are also limits on the law, as well as different legal traditions in Canada including Indigenous legal traditions and religious laws. These also impact on professional standards, where there are competing views about the potential conflict between legal and medical conceptions about rights and care. This is an important questions for this project, and illustrate how law reform is relevant to what may be perceived as medical, administrative or public policy issues in the last stages of life.
| 3. | What legal rights and principles are important for shaping care and establishing professional standards in the last stages of life? |
Ontario’s Laws, Policies and Programs (chapter 4): Laws, policies and programs create a framework defining several core aspects of the last stages of life in Ontario: the approach to and delivery of palliative care services; health-care decision making, planning, and substitute consent; medical assistance in dying; and resolving health care disputes. A considerable amount of discussion is taking place around key controversies in these areas, including a “public health” approach to palliative care, access to palliative care, and access to medical assistance in dying. In addition to these there are other laws which also intersect with medical assistance in dying, raising issues related to capacity assessments, transitions in care, employment concerns, caregiver benefits, insurance coverage, and rights in long-term care and retirement homes.
| 4. | Legislation governing health care, housing, employment, professions, and other areas intersects with the last stages of life – what gaps exist that would benefit from greater certainty or clarity? |
| 5. | Should a public health approach to palliative care be integrated into Ontario’s regulatory framework, and how would it look on the ground? |
| 6. | The LCO has identified several areas where medical assistance in dying could be clarified, including transitions in care, conscientious objection, and appeals of capacity determinations. Are there other additional issues to consider? |
Access to Justice for Communities with Unmet Needs (chapter 5): Recent government reviews of palliative care confirm that Ontarians suffer marked disparities in accessing quality care in the last stages of life.[9] LCO has particularly identified unmet needs respecting different communities. These include caregivers and other families and friends; persons living in long-term care and retirement homes; First Nations, Inuit and Métis people; persons experiencing homelessness; persons with disabilities; and faith and culturally diverse communities. There are various strategies, controversies, options, and choices in terms of accommodating these diverse communities.
| 7. | What are your experiences as a member or supporter of a community of need going through the last stages of life? |
| 8. | What law reforms do you believe are needed for communities with unmet needs, and how would such reforms be most effectively implemented in law? |
| 9. | Are there any communities with unmet needs who are not identified in this paper that the LCO should consider? |
Specific Challenges to Accessing Care in the Last Stages of Life (chapter 6): This chapter considers issues related to autonomy, self-determination, beneficence (and maleficence) in care, and safeguards against abuse. These arise in several specific contexts, including the legal framework for, and public understanding of, consent and advance care planning; decision-making authority over life-sustaining practices, including withdrawal and withholding of treatment, CPR, and nutrition; palliative sedation therapy; managing planned deaths at home; the experience of supporting professionals; and accommodation and supports for faith and cultural communities. Unclear legal regulation of these issues leads to uncertainty and conflict, but must also contend with difficult controversies related to who has decision making authority in critical situations.
| 10. | How can institutions, professionals and the public be better supported to obtain meaningful and legally compliant health care consent? |
| 11. | How can practice tools achieve the goal of providing accurate, consistent and meaningful information about consent and advance care planning? |
| 12. | There are connecting laws, principles and policies regarding decision making for life-sustaining practices such as CPR, DN, and nutrition. What are the strengths, weaknesses and gaps in Ontario’s current legal framework for decision-making authority over life-sustaining practices? |
| 13. | Who should have authority to determine whether life-sustaining and lifesaving treatment (e.g., CPR, DNR) is offered to, or withdrawn from, a patient – the patient (or SDM) or a health care provider? Under what circumstances? |
| 14. | Should Ontario regulate the offering of food and water to persons nearing the end of life, including the authority of SDMs to consent to withholding necessities of life? |
| 15. | Should Ontario regulate the clarity, consistency and safety of palliative sedation therapy considering the ethical challenges, medical assistance in dying, and the need for safeguards like informed consent? |
| 16. | Which options are preferred to better plan for and manage expected deaths at home? Would it be beneficial to have a province-wide strategy or formal regulation? |
| 17. | How can strategies for addressing the needs of health care providers assist with mental and moral stress? How can health care practitioners be better prepared to manage disputes? |
| 18. | Do legal professionals require specific education and guidance on matters relating to the last stages of life, and what form might this best take? |
| 19. | What approaches are best suited to address barriers, accommodations and supports to better integrate faith, cultural and spiritual practices into care nearing the end of life? |
Assistance with the Law: Navigation, Dispute Resolution and Public Legal Education (chapter 7): The illness trajectory for each person is unique – it may be long or brief, stable or fluctuating. Care may be provided to persons in their own homes through community-based services; long-term care and retirement homes; hospital departments; and in residential hospices. However, many Ontarians experience problematic transitions and may face barriers to accessing services like medical assistance in dying. It can also be unclear and confusing where to turn when disputes arise.
| 20. | What are your experiences as a patient or caregiver transitioning between care settings in the last stages of life? |
| 21. | Are law reform measures needed to improve access, navigational supports, and the coordination of care within the health care system? |
| 22. | What strategies, processes, or institutions are best suited to resolving disputes in the last stages of life? |
| 23. | How can legal information or education about the law be made more relevant, timely, and effective in the last stages of life? |
D. The project scope incorporates ongoing developments
This project was initiated following a request from the Registered Nurses’ Association of Ontario (RNAO) that the LCO study medical assistance in dying in Ontario. The LCO Board of Governors approved the project in 2014, prior to the Supreme Court of Canada’s decision in Carter v. Canada (Attorney General), which found certain Criminal Code provisions prohibiting physician-assisted dying to be unconstitutional.[10] Since the release of the Supreme Court’s decision, the federal and provincial governments have taken measures to delineate the availability of medical assistance in dying, the procedural requirements for its delivery, and the respective rights and responsibilities of various parties.
Parliament amended the Criminal Code to define eligibility criteria and protect those involved in the practice in specific circumstances.[11] At the provincial level, the Ontario government introduced measures to clarify how medical assistance in dying is to be delivered in practice as well as the process for conscientiously objecting providers to make effective referrals, among other measures. Regulatory health colleges have also published guidance for their members. (More information on the legal framework for medical assistance in dying is found in chapter 4, “Ontario’s Laws, Policies and Programs”.)
Furthermore, after the LCO’s project began, the Ontario Government made a number of public commitments to support a comprehensive strategy on palliative care.[12] One of these commitments included the launch of a provincial network called the Ontario Palliative Care Network (OPCN). The OPCN brings together a broad range of partners, to drive implementation of consistent quality hospice palliative care across the province.[13] The LCO is aware that the OPCN will be addressing systemic barriers relating to Ontario’s decentralized institutional framework which may go a long way in bridging disparities in access.
In addition to these non-legislative measures, on May 10, 2017, the government of Ontario introduced Bill 84, the Medical Assistance in Dying Statute Law Amendment Act, 2016.[14] Bill 84 aligns with the federal MAID legislation (Bill C-14, An Act to amend the Criminal Code and to make related amendments to other Acts (medical assistance in dying)), to address areas relevant to MAID that fall under provincial jurisdiction.
Throughout our planning for this project, the LCO has sought to be sensitive to government activities in these two areas, which materialized after our own project was approved. The LCO strives to prevent overlap between our work and contemporaneous initiatives in all of our projects. However, avoiding overlap is distinctly important in this instance because the federal and provincial governments’ planning is evolving and in a state of development. The LCO will, however, address issues and bridge gaps that complement these initiatives and inform their development from a legal perspective.
For greater clarity, the following determinations have been made regarding LCO’s scope for this project:
Ø The LCO will not address matters of clinical practice. During background consultations we asked stakeholders about limitations on the LCO’s project. We were advised not to address matters of clinical practice, and we agree. The LCO views the analysis of health care providers’ scope of practice as falling outside our mandate as a law reform agency. The LCO’s definition of “last stages of life” is unique; it distinguishes the experience of persons who are dying – as a particular stage in life – from established models of care that may beneficial during the dying process, most notably palliative and end-of-life care.
Similarly, our definition of “care” is broad; it encompasses various services and supports that could be provided during the last stages of life, including medical treatments (and offering, withdrawing and withholding such treatment); accompaniments (e.g., psychological, social and spiritual counselling); and daily living assistance (e.g., bathing, cooking and dressing). The definition of “care” used in this document recognizes service and supports for caregivers, family and friends, such as respite and bereavement counselling. It is also closely connected to legal assistance and navigational supports that may indirectly affect access to care. It does not include matters of clinical practice.
Ø LCO will not address challenges in education for medical and legal professionals. During background consultations the LCO received many comments from members of the public about several challenges that health care providers face in providing palliative care. The foremost challenges that were identified were the lack of moral supports for psychological distress, lack of clinical education (for primary and specialty care providers), and the desirability of expanding aspects of registered nurses’ scope of practice to increase accessibly to a range of services (e.g., medications, death certifications, treatments).
Of these issues, the LCO’s project will only address health care providers’ employment-related psychological supports for a number of reasons. First, as above, the LCO will not address matters of clinical practice. Second, the LCO does not wish to duplicate ongoing efforts of the Ministry of Health and Long-term Care and the OPCN to strengthen education for health care providers.
Legal professionals also face a variety of challenges when it comes to advising clients who are dying and those around them. Similar to our approach to health care providers, this project does not consider challenges with education for legal professionals on decision-making issues due to our work on that subject in the Legal Capacity, Decision-Making and Guardianship project (see section D, below).
Ø For our discussion about the challenges legal and medical professions face in providing palliative care and services see chapter 6.F, “Understanding the experiences of supporting professionals”.
Ø The LCO will not duplicate federal and provincial work on medical assistance in dying. The actions taken, initiatives proposed, and measures introduced by the federal and provincial governments to date were further clarified in December 2016. Ontario’s introduction of Bill 84 addressed several amendments to the Coroner’s Act, Vital Statistics Act, Excellent Care for All Act, Municipal / Freedom of Information and Protection of Privacy Act, and the Workplace Safety and Insurance Act. Additionally, the federal government announced that the Council of Canadian Academies will conduct independent reviews of medical assistance in dying requests “relating to requests by mature minors, to advance requests, and to requests where mental illness is the sole underlying medical condition”. These efforts greatly clarify which issues the LCO should address in this project as complimentary to or beyond the scope of these government initiatives, and without repeating those initiatives.
Ø For more information on medical assistance in dying and palliative care in Ontario, see chapter 2.B, “Recent Policy Debates about Rights Nearing the End of Life” and chapter 4.E, “Medical assistance in dying”.
Ø The LCO will rely on findings from past and ongoing projects. This discussion paper draws on findings from several of the LCO’s past and ongoing projects, the most notable of which are explained below in section D. Key issues reviewed in these earlier projects include recommendations regarding laws in Ontario on informed consent, advance care planning and substitute decision-making; professional education and rules of professional conduct; and formal dispute resolution mechanisms, particularly the Consent and Capacity Board.
E. The LCO’s approach to law reform
1. Our mandate and values
The LCO is Ontario’s leading law reform agency. The core of our mandate is fostering “access to justice,” which we aim to achieve by undertaking rigorous research and analysis, disseminating reports and engaging in critical debate, among other activities. The LCO recognizes that “[a] more comprehensive understanding of access to justice goes beyond the legal system to encompass efforts to assess and respond to ways in which law impedes or promotes economic or social justice”.[15]
LCO reports include principled, practical, “problem-solving” recommendations informed by broad consultations and tested through a transparent, comprehensive review process that engages a broad range of individuals, experts, and institutions. The LCO gives a voice to marginalized communities and others who should have an important role in law reform debates and discussions.
The LCO has developed a comprehensive project development, research and consultation strategy to organize our work. This strategy ensures that the LCO’s projects are transparent and participatory. LCO projects are delivered in several phases that are typically concentrated around the release of three core documents: a discussion paper, interim report and final report. Below we describe the research and consultations we have conducted to date in preparing this discussion paper.
2. Project development, research and consultations
a. Preliminary Research and Consultations
The discussion paper was drafted following considerable research and consultations beginning in April 2015. Preliminary research involved an environmental scan of literature in disciplines including law, medicine and the social sciences as well as a review of government and other policy documents. Our preliminary consultations consisted of nearly 70 semi-structured interviews with individuals and organizations, representing wide-ranging perspectives. We consulted an additional 35 participants in a large stakeholder event (see below), raising our preliminary consultations to over 100 individuals and organizations. The issues addressed in this paper are grounded in our consultation results as well as our initial research.
Ø A list of individuals and organizations we have consulted is found at Appendix B
This discussion paper also draws on findings from several of the LCO’s past and ongoing projects.
Most notably, it relies on LCO reports regarding capacity and decision-making, older adults and persons with disabilities:
Legal Capacity, Decision-Making and Guardianship: Since the end of 2012, the LCO has led a law reform project that comprehensively reviews and assesses Ontario’s regulatory framework for legal capacity and decision-making. It examines three interlocking statutes: the Substitute Decisions Act, 1992 (SDA), the Health Care Consent Act, 1996 (HCCA) and certain provisions in the Mental Health Act.[16] In March 2016, we released an Interim Report with draft recommendations.[17]
Ø The final report was released in March 2017, and is available online at http://www.lco-cdo.org/en/capacity-guardianship
A Framework for the Law as it Affects Older Adults: This project defines a set of principles to guide the evaluation and development of laws, policies and programs in order to take into account the experiences of older adults, and to promote positive outcomes for older adults as full members of society.[18]
Ø The final report was released in April 2012, and is available online at http://www.lco-cdo.org/en/content/older-adults
A Framework for the Law as it Affects Persons with Disabilities: This project defines a set of principles to guide the evaluation and development of laws, policies and programs in order to take into account the experiences of persons with disabilities, and to promote positive outcomes for persons with disabilities as full members of society.[19]
Ø The final report was released in September 2012, and is available online at http://www.lco-cdo.org/en/content/persons-disabilities
These projects are relevant to many of the individuals and communities affected by this current project.
For example, the LCO’s “Framework” projects address the communities of older adults and persons with disabilities, both of whom are uniquely affected by care in the last stages of life. The Framework projects also recognize the importance of autonomy, dignity and security as well as the need to balance tensions between these principles. Tensions between these principles underpin current debates on rights to palliative care and medical assistance in dying – to mention but a few issues this discussion paper examines. Additionally, the LCO’s Frameworks are consistent with other principles-based frameworks and statements being produced by the courts, government agencies, professional associations and research institutes on rights nearing the end of life.[20]
This project is also related to the LCO’s recently completed Legal Capacity, Decision-Making and Guardianship project. The capacity and decision-making project has developed recommendations regarding laws in Ontario on informed consent, advance care planning and substitute decision-making, which are all relevant to the last stages of life.
Accordingly, this paper does not repeat our research and analysis in the LCO’s capacity and decision-making project; instead, it relies on findings in that project, where appropriate.
Ø To access reports and other documents from the LCO’s past and ongoing projects, please visit our website at http://www.lco-cdo.org/.
b. Advisory Group
In September 2015, the LCO formed an Advisory Group for the project. The purpose of the Advisory Group is to provide the LCO with advice throughout the project. Advisory Group members include representatives of the Ministry of the Attorney General (MAG), MOHLTC, academics, bioethicists, physicians, nurses, personal support workers, psychologists, trusts and estates lawyers, legal clinics, professional associations, residential and visiting hospices, and advocacy organizations. A number of the Advisory Group members are respected specialists in palliative and end-of-life care and in legal frameworks relevant to death and dying.
The Advisory Group gave the LCO helpful input into the structure and content of our documents, beginning with the project scope released in January 2016. It then reviewed this discussion paper and provided the LCO with significant feedback. We are incredibly grateful for the Advisory Group members’ invaluable observations and commitment.
Ø A list of Advisory Group members is provided at Appendix C
c. Commissioned Research Papers
The LCO benefited from seven research papers that we commissioned from multidisciplinary teams especially for this project and from research papers previously completed for our Legal Capacity, Decision-Making and Guardianship project. These papers are available publicly at www.lco-cdo-org. The authors’ findings and suggestions have been taken into account in our analysis to date, although the views expressed in them do not necessarily reflect the views of the LCO. These commissioned papers are as follows.
- Judith Wahl (Advocacy Centre for the Elderly), Mary Jane Dykeman (Dykeman Dewhirst O’Brien LLP) & Tara Walton: Informed consent, advance care planning and substitute decision-making: using practice tools to ensure meaningful decision-making in the last stages of life
- Dr. Donna Wilson & Dr. Stephen Birch: Improved care setting transitions in the last year of life
- Dr. Mary Chiu, Dr. Adrian Grek, Sonia Meerai, LJ Nelles, Dr. Joel Sadavoy & Dr. Virginia Wesson: Understanding the lived experience of individuals, caregivers and families touched by frailty, chronic illness and dementia in Ontario
- Omar Ha-Redeye, Ruby Latif & Dr. Kashif Pirzada: Integrating religious and cultural supports into quality care in the last stages of life in Ontario
- Susan Brown, Dr. James Downar, Dr. Jennifer Gibson, Dr. Laura Hawryluck, Dr. Csilla Kaloscai, Dr. Joy Richards, Robert Sibbald & Alexi Wood: Balancing the interests of patients, substitute decision-makers, family and health care providers in decision-making over the withdrawal and withholding of life-sustaining treatment
- Dr. Arne Stinchcombe, Dr. Katherine Kortes-Miller & Dr. Kimberley Wilson: Perspectives on the final stage of life from LGBT elders living in Ontario
- Sandy Buchman, Rosario Cartagena, Rose Geist, Mark Handelman, Kaveh Katebian, Wendy Lawrence, Trudo Lemmens, Harvey Schipper, Gilbert Sharpe & Alison Thompson: The impact of suffering on decision-making and methods of assessing capacity in the last stages of life
Ø Additional information about research papers commissioned for the LCO’s project are listed in Appendix D. The papers are available online at http://www.lco-cdo.org/en/last-stages-of-life
d. Roundtable on Legal Ethics and Practice for the Last Stages of Life
The LCO co-hosted the Roundtable on Legal Ethics and Practice for the Last Stages of Life with our valued partners listed in Appendix E. This consultation brought together about 35 legal experts to discuss common challenges the profession faces and options for reform. Participants included academics, government lawyers, and members of the judiciary, the Law Society of Upper Canada, regulatory health colleges, and the trusts and estates bar. Information from the session was incorporated into this discussion paper.
Ø Further information on the Roundtable on Legal Ethics and Practice for the Last Stages of Life can be accessed through our project webpage at http://www.lco-cdo.org/en/last-stages-of-life
F. How to Participate
The LCO’s approach to law reform is driven by public consultation. We take a multidisciplinary approach to research that involves the participation of individuals, communities and institutions across the province. Learning about your experiences and opinions is critical to our analysis of options for law reform.
The full Discussion Paper is the first step in facilitating this engagement. The paper is designed to explain the project’s scope, outline the LCO’s methodology, identify key issues and provide information on how the public can participate in the project. We’ve also summarized other issues in a Consultation Issues Map and Issue Backgrounders, available on our website.
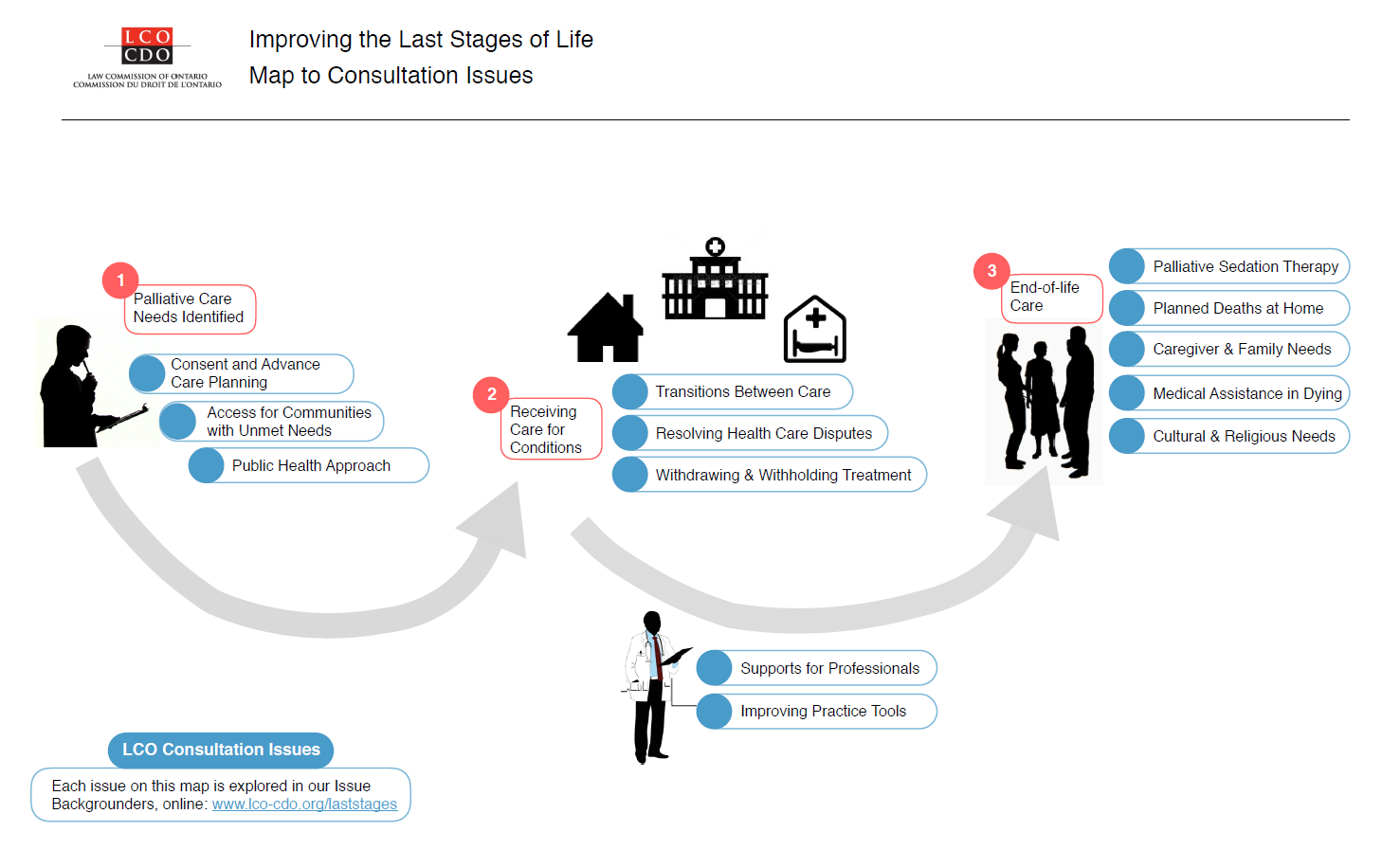{kind=link}
LCO’s formal consultation period runs from May – September 2017. The LCO invites your participation through:
- The project website at http://www.lco-cdo.org/laststages
- Written submissions at any time to lawcommission@lco-cdo.org
- Watch live and archived webcast consultation sessions
- Complete the consultation survey on your mobile, tablet, or computer
- Propose an in-person focus group for your community
- Contacting Project Research Lawyer Ryan Fritsch through the contact information below
Send your comments to:
Law Commission of Ontario Toronto (416) 650-8406
Project on Improving the Last Stages of Life Toll-Free (866) 950-8406
2032 Ignat Kaneff Building Fax (416) 650-8418
Osgoode Hall Law School, York University E-mail: lawcommission@lco-cdo.org
4700 Keele Street, Toronto, ON M3J 1P3
Written submissions will be accepted until September 29, 2017
[1] See for example: “Palliative Care” in Auditor General of Ontario, Annual Report 2014 (Toronto: Queen’s Printer for Ontario, 2014), 260 [AG 2014], which reports that: “People aged 85 and over constituted the fastest-growing segment of Ontario’s population between 2006 and 2011, with their number increasing by 29% over that period. The number of people aged 65 and over is expected to more than double from 2 million in 2012, when baby boomers began to turn 65, to over 4 million by 2036, when seniors will constitute 24% of Ontario’s population.”
[2] See for example: Allison Williams, Mary Lou Kelley, Sarah Dykeman & Lily DeMiglio, A Timeline of Hospice Palliative Care Policy and Practice in Ontario, Canada (Canadian Institute of Health Research, February 2010), 3 [Williams]; Francois-Pierre Gauvin, Julia Abelson, John N. Lavis, Citizen Brief: Improving Access to Palliative Care in Ontario (Hamilton, Canada: McMaster Health Forum, 16 November 2013), 2 [Gauvin].
[3] Statistics Canada, “Deaths, estimates, by province and territory, 2011/12 – 2015/16”, online: http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/demo07a-eng.htm (last accessed January 13, 2017).
[4] Ontario Ministry of Health and Long-term Care, “Hospitals: Questions and Answers”, online: http://www.health.gov.on.ca/en/common/system/services/hosp/faq.aspx#hospitals (last accessed January 13, 2017). The proportion of Ontarian’s dying in hospital is found in Donna Wilson & Steven Birch, Improving End-of-Life Care Setting Transitions: A Mixed-Method Research Report (report commissioned by the Law Commission of Ontario, 2016), 31.
[5] S Baidoobonso, Effect of Supportive Interventions on Informal Caregivers of People at the End of Life: A Rapid Review (Toronto: Health Quality Ontario, 2014) [Baidoobonso], 7.
[6] Ontario Long-term Care Association, “Sector Dashboard – Ontario (updated October 2016),” online: http://www.oltca.com/OLTCA/Documents/Sector%20Dashboards/Ontario_Dashboard_1016.pdf (last accessed January 13, 2017).
[7] CTV News, “At least 744 assisted-deaths in Canada since law passed: CTV News analysis” (December 28, 2016), online: http://www.ctvnews.ca/health/at-least-744-assisted-deaths-in-canada-since-law-passed-ctv-news-analysis-1.3220382 (last accessed January 13, 2017).
[8] Law Commission of Ontario, “Improving the Last Stages of Life: Project Scope Statement”, online: http://www.lco-cdo.org/en/last-stages-of-life-project-scope (last accessed 25 July 2016).
[9] On the adequacy of palliative care in Ontario, see AG 2014, note 1, ch. 3. There are also centres of excellence in Ontario and many initiatives that are ongoing to strengthen palliative care as discussed later in this discussion paper. On centres of excellence, see: Canadian Medical Association, Palliative Care: Canadian Medical Association’s National Call to Action (May 2015), online: https://www.cma.ca/Assets/assets-library/document/en/advocacy/palliative-care-report-online-e.pdf (last accessed March 21, 2017). For information on ongoing initiatives in Ontario, see chapter 4, “Ontario’s Laws Policies and Programs”.
[10] Carter v. Canada (Attorney General), [2015] 1 SCR 331 [Carter].
[11] Parliament of Canada, Bill C-14, An Act to Amend the Criminal Code and to Make Related Amendments to Other Acts (Medical Assistance in Dying), 1st Sess., 42nd Parliament, 2015-2016 (assented to June 16, 2016) [Bill C-14], online: http://www.parl.gc.ca/LegisInfo/BillDetails.aspx?Language=E&Mode=1&billId=8177165 (last accessed 25 July 2016).
[12] Government of Ontario, “Province Strengthens End-of-Life Care with $75 Million Investment” [Ontario 2016], online: https://news.ontario.ca/mohltc/en/2016/03/province-strengthens-end-of-life-care-with-75-million-investment.html (last accessed 25 July 2016).
[13] Ontario 2016, note 12. See also Cancer Care Ontario, “The Ontario Palliative Care Network”, online: https://www.cancercare.on.ca/pcs/palliative/opcn/ (last accessed 25 July 2016).
[14] Government of Ontario, Bill 84, Medical Assistance in Dying Statute Law Amendment Act, 2017, 2nd Sess., 41st Parliament, 2016-2017 (first reading December 7, 2016), online: http://www.ontla.on.ca/web/bills/bills_detail.do?locale=en&BillID=4460&detailPage=bills_detail_status (last accessed March 13, 2017).
[15] Law Commission of Ontario, Increasing Access to Family Justice through Comprehensive Entry Points and
Inclusivity (Toronto: February 2013), 15, online: http://www.lco-cdo.org/family-law-reform-final-report.pdf (last accessed 25 July 2016).
[16] Health Care Consent Act, 1996, S.O. 1996, c.2 [HCCA]; Substitute Decisions Act, 1992, S.O. 1992, c.30 [SDA]; Mental Health Act, R.S.O. 1990, Ch. M.7 [MHA].
[17] Law Commission of Ontario, Legal Capacity, Decision-making and Guardianship: Interim Report (Toronto: Law Commission of Ontario, October 2015), online: http://lco-cdo.org/en/capacity-guardianship-interim-report (last accessed 25 July 2016).
[18] Law Commission of Ontario, A Framework for the Law as It Affects Older Adults: Advancing Substantive Equality for Older Persons through Law, Policy and Practice (Toronto: April 2012), online: http://lco-cdo.org/en/content/older-adults (last accessed 25 July 2016).
[19] Law Commission of Ontario, A Framework for the Law as It Affects Persons with Disabilities: Advancing Substantive Equality for Older Persons through Law, Policy and Practice (Toronto: April 2012), online: http://lco-cdo.org/en/content/persons-disabilities (last accessed: 25 July 2016).
[20] See for instance: Nadia Incardona, Sally Bean, Kevin Reel & Frank Wagner, An Ethics-based Analysis and Recommendations for Implementing Physician-Assisted Dying in Canada (Toronto: Joint Centre for Bioethics, University of Toronto, 2016); Cuthbertson v. Rasouli, [2013] 3 SCR 341 [Rasouli]; Carter, note 10; Canadian Medical Association, Principles-based Recommendations for a Canadian Approach to Assisted Dying (January 2016), online: https://www.cma.ca/Assets/assets-library/document/en/advocacy/cma-framework_assisted-dying_final-jan2016-edited-20160412.pdf (last accessed 25 July 2016); Canadian Hospice Palliative Care Association, Quality End-of-Life Care Coalition of Canada & Government of Canada, The Way Forward: A Roadmap for an Integrated Palliative Approach to Care (March 2015), 13 [The Way Forward].