
What is the Last Stages of Life Project?
The Law Commission of Ontario (LCO) is Ontario’s leading law reform agency. The goal of our Improving the Last Stages of Life project is to identify and recommend law reforms in the “last stages of life.” This is a broad and inclusive term that allows us to look at rights and legal issues in end-of-life planning, palliative care, medical assistance in dying, and other issues. An important aspect of this is Consent and Advance Care Planning (ACP), the subject of this backgrounder. This backgrounder is one of a series of consultation documents the LCO has developed for this project.
This document is a brief overview intended to raise issues and stimulate discussion for the purposes of LCO’s consultations. This document should not be relied on as a source of law.
Why is Consent and Advance Care Planning Important in the Last Stages of Life?
Persons in the last stages of life may not have the ability (capacity) to direct (consent) to their health care at all times. ACP can play an important role in these circumstances.
ACP is a process that involves a person identifying and choosing a substitute decision maker(s) (SDM), and sharing the wishes, values and beliefs that an SDM must interpret when making decisions on the person’s behalf. The LCO has adopted the definition of advance care planning used by the Hospice Palliative Care Ontario Health Care Consent Advance Care Planning Community of Practice (April 2016). Importantly, consent and ACP relies on legislation specific to Ontario. Approaches in other jurisdictions or provinces may be different.
Research and experience has proven that advance care planning conversations improve patient and family satisfaction with end-of-life care. These processes aim to ensure alignment between a person’s values and treatment; lessen family distress; decrease hospitalizations and admissions to critical care; and decrease unwanted investigations, interventions and treatments, among other benefits.
If no SDM has been identified and chosen in advance, legislation sets out a hierarchy of people who can act as SDMs. In descending order of rank, the list names: guardians of the person; an attorney named in a power of attorney for personal care; representatives appointed by the Consent and Capacity Board (CCB); a spouse or partner; a child or parent; a sibling; and finally, “any other relative.” Together, the Health Care Consent Act, 1996 and Substitute Decisions Act, 1992 govern informed consent, advance care planning and substitute decision-making in Ontario.
How does Advance Care Planning work with health care consent?
In Ontario, ACP refers to a specific set of processes and legal issues that can take place at any time, including during the last stages of life. It is therefore important to distinguish ACP from the following:
- ACP does not constitute consent to treatment. The law in Ontario states that, except in emergencies, health care providers must always obtain consent from an individual or an incapable individual’s SDM, prior to administering treatment, even if the individual has engaged in ACP. The law further states that when substitute consent is required, the person’s known wishes, values and beliefs must guide the SDMs’ decision-making process. If these are unknown, the incapable individual’s SDM must interpret the wishes, values and beliefs of the individual.
- ACP is often confused or conflated with other concepts. As stated earlier, informed consent and ACP are specific to Ontario’s consent legislation. Nonetheless, concepts or approaches that may be used in other jurisdictions – such as “advance directives” or “living wills” – may wrongly be invoked. These are terms which are not legally defined in Ontario, and so can cause confusion. Similarly, terms like “goals of care” can assist both health care providers and decision-makers explore which treatments and care decisions are best aligned with these goals, but as person-focused precursors to informed consent and decision-making.
- ACP is not the same as “do not resuscitate” or “no CPR” notes. These kinds of treatment decisions require consent. ACP can be used to identify wishes, values and beliefs to guide SDMs in their decision making. DNR and CPR situations are discussed in greater detail in LCO’s Discussion Paper (ch. 6.C) and Issue Backgrounder #4 “Withdrawing and Withholding Treatment.”
- ACP does not replace consent in medical assistance in dying. The requirement for consent immediately before receiving MAID restricts individuals from making a MAID request in advance through an advance care planning document. This issue of “advance requests” is under review by the Council of Canadian Academies, at the direction of the Federal Government.
Where can I get more detailed information on this topic?
The LCO’s Improving the Last Stages of Life Discussion Paper (May 2017) discusses the law and practices around consent and ACP in greater depth. Specifically, see the discussion at chapter 4.D and 6.B. Please also see the findings and recommendations made in the LCO’s recently completed Legal Capacity, Guardianship and Decision-Making Final Report (March 2017).
What kinds of questions is the LCO asking?
The LCO’s recent and comprehensive project on Legal Capacity, Guardianship and Decision-Making considered many issues relevant to ACP. This project takes this analysis further, and considers the use of ACPs specifically within the context of the last stages of life. Issues that the LCO is considering include:
- ACP and decisions about life-saving or life-sustaining treatment. While consent must be obtained to withdraw treatment from a person who is already being treated, the law is unsettled as to whether providers can legally withhold treatment by simply not offering it to the patient or SDM from the outset (or by refusing to provide it on request) when, in the health care provider’s opinion, life-supports would be of little or no “beneficial” value. Can ACP play a role in decreasing conflicts, including consideration of cultural values, misunderstandings about consent, and disagreements over life-saving treatments? Can specific approaches to ACP better assist SDMs in interpreting values, beliefs and wishes?
- The development of better consent and ACP tools and information. LCO has heard widespread concerns about misunderstandings of the law, and shortcomings in its implementation, in relation to the last stages of life. What are your experiences with public information and practice tools? Given the wide array of practice tools that have been created for various contexts, how can the provision of accurate, consistent and meaningful information about consent and advance care planning be ensured? Is it desirable or possible to create standardized practice tools across Ontario? Should there be a systemic approach that better supports the consistent use of legally compliant terminology, education and enforcement? Can existing efforts be scaled up? Can good communication and goals of care discussion be better integrated into preparing for decision-making? How can institutions, professionals and the public be better supported to obtain meaningful and legally compliant health care consent?
- Can more be done to support patients? The process of discussing ACP may include conversations about informed consent and rights that can be confusing. Is there a need for greater or systematized supports to provide information to patients? DO you feel there is an effective way to achieve this, such as a system of providing rights information, or delegating an institution with supporting a strategy for outreach and education? Would SDMs be better empowered if they were obligated to be informed of their roles and responsibilities?
How can I share my views on this issue?
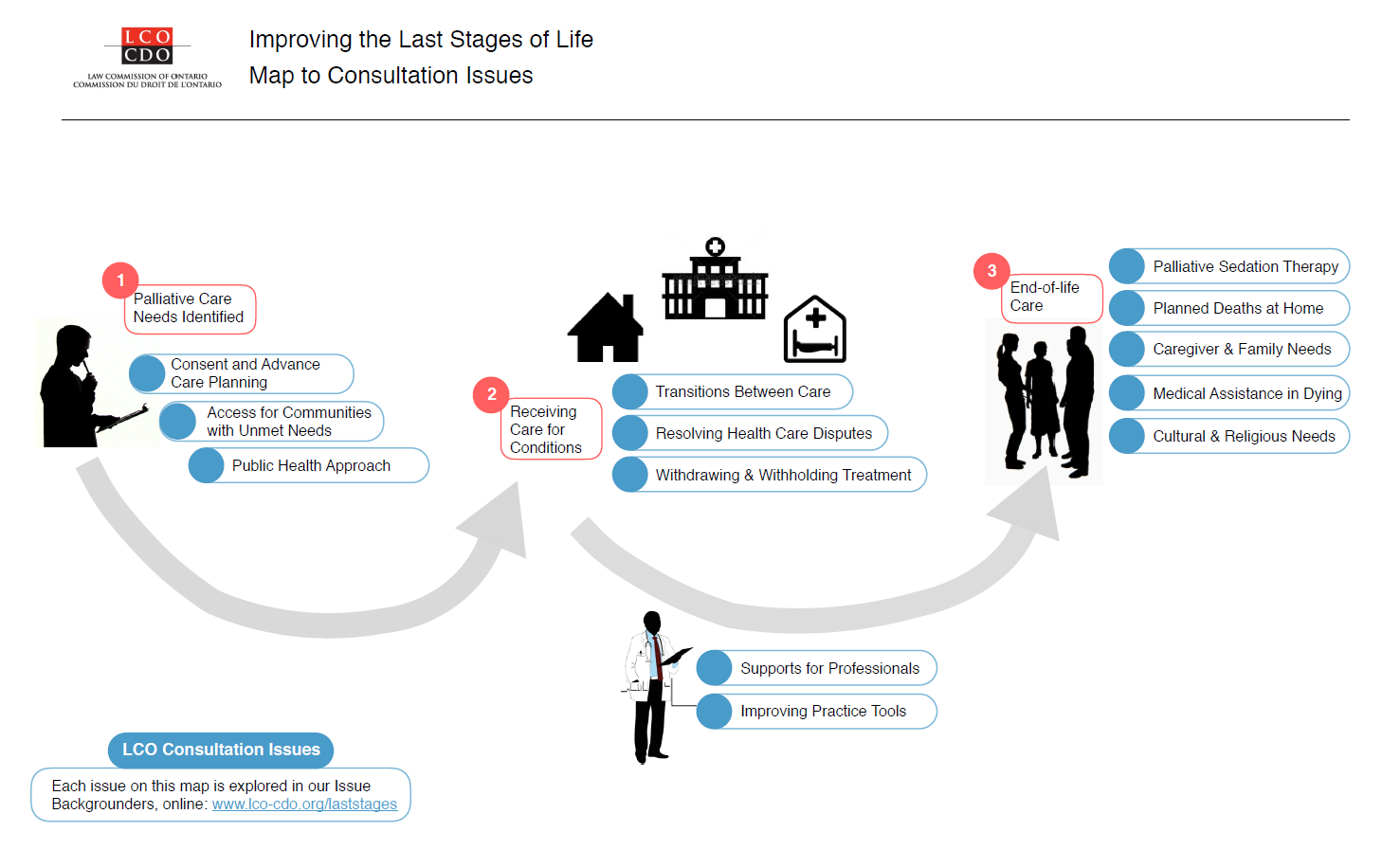
A fuller examination of these issues is available in our Executive Summary and Discussion Paper. We’ve also summarized other issues in a Consultation Issues Map and additional Issue Backgrounders.
{kind=link}
LCO’s formal consultation period runs from May – September 2017. The LCO invites your participation through:
- The project website at http://www.lco-cdo.org/laststages
- Written submissions at any time to lawcommission@lco-cdo.org
- Watch live and archived webcast consultation sessions
- Complete the consultation survey on your mobile, tablet, or computer
- Propose an in-person focus group for your community
- Contacting Project Research Lawyer Ryan Fritsch through the contact information below
Law Commission of Ontario Toronto (416) 650-8406
Project on Improving the Last Stages of Life Toll-Free (866) 950-8406
2032 Ignat Kaneff Building TTY (416) 650-8082
Osgoode Hall Law School, York University Fax (416) 650-8418
4700 Keele Street, Toronto, ON M3J 1P3 E-mail: lawcommission@lco-cdo.org
Written submissions will be accepted until September 29, 2017