
What is the Last Stages of Life Project?
The Law Commission of Ontario (LCO) is Ontario’s leading law reform agency. The goal of our Improving the Last Stages of Life project is to identify and recommend law reforms in the “last stages of life.” This is a broad and inclusive term that allows us to look at rights and legal issues in end-of-life planning, palliative care, medical assistance in dying, and other issues. An important aspect of this is establishing a public health approach to palliative care, the subject of this backgrounder. This backgrounder is one of a series of consultation documents the LCO has developed for this project.
This document is a brief overview intended to raise issues and stimulate discussion for the purposes of LCO’s consultations. This document should not be relied on as a source of law.
How did medical assistance in dying develop in Canada?
In 2015, the Supreme Court of Canada released its landmark decision in Carter v. Canada, overturning criminal sanctions against physician assisted dying. The Court found that physician assisted dying is available to competent adults who consent to the termination of life and who have a grievous and irremediable medical condition that causes enduring, intolerable suffering to the individual. In June 2016, the federal government implemented legislation to regulate “medical assistance in dying.” “Medical assistance in dying” or “MAID” is now the preferred term in Canada because it recognizes that, in practice, this service is being delivered in teams of health care providers, not only by physicians.
MAID is now an accepted practice across Canada. As of December 2016, media outlets reported that some 744 medically assisted deaths occurred across Canada since legislation went into effect that year, of which 180 took place in Ontario.
How is medical assistance in dying delivered in Canada?
Medical assistance in dying can be delivered in two ways:
- A physician or nurse practitioner can administer a substance that causes death to a person at that person’s request.
- A person can self-administer the substance obtained with a physician or nurse practitioner’s prescription.
The Criminal Code exempts individuals involved in the process from criminal liability, including the physician, nurse practitioner, pharmacists, and anyone who does anything to aid them, including anyone who aids the patient to self-administer at the patient’s request.
The Criminal Code also now explicitly sets out eligibility criteria, procedural requirements and safeguards against abuse. Persons who are eligible for medical assistance in dying must be entitled to Canadian health insurance, be at least 18 years old, make a voluntary request, give informed consent and have a grievous and irremediable medical condition. A “grievous and irremediable medical condition” is further defined to limit eligibility to persons who are dying – which is to say that their natural death is “reasonably foreseeable.” These criteria exclude individuals who may suffer as a result of physical or mental conditions, but who are not dying.
MAID legislation also commits the federal government to study three special cases: issues relating to MAID requests by mature minors under 18 years of age; to advance requests or “advance directives” that would authorize MAID when the person became incapable; and to MAID requests where mental illness is the sole underlying medical condition. The government announced in December 2016 that the Council of Canadian Academies will conduct independent reviews related to these specific types of requests and deliver a final report to Parliament in December 2018.
How is medical assistance in dying defined in Ontario?
Because federal legislation serves to create exemption to the Criminal Code, it is up to the provinces to define how health care services will be defined on the ground.
In Ontario, the Ministers of the Attorney General and Health and Long-term Care worked together to clarify that patients should consult directly with their health care providers about medical assistance in dying and, in turn, health care providers should consult their regulatory colleges about any rules, guidelines or practices.
Several of these professional colleges have now developed guidelines that speak to issues including MAID eligibility, capacity assessments, voluntariness and informed consent, and documentation and reporting requirements.
One particular issue concerns “conscientious objection.” The College of Physicians and Surgeons (CPSO) Policy on MAID, for instance, directs that “Where a physician declines to provide medical assistance in dying for reasons of conscience or religion, the physician must not abandon the patient. An effective referral must be provided.”
Ontario established a Clinician Referral Service to assist physicians in making an effective referral for consultation and assessment for possible medical assistance in dying cases. This includes a roster of physicians willing to provide MAID services.
Neither federal nor provincial legislation compels physicians to provide or assist in providing MAID, and the CPSO has clarified that it does not consider “providing the patient with an “effective referral” as “assisting” in providing MAID.” Nonetheless, some professionals see that as the case and are urging greater clarity on the issue.
Ontario also recently re-iterated its commitment to give patients direct access to a proposed care coordination service for MAID. The system is said to model that in Alberta, which has provincial care coordinators who respond to patient requests for MAID via phone or email. They help patients complete necessary paperwork, find doctors to perform the eligibility assessment, and help arrange the assisted death itself. Some Ontario hospitals have also created their own assisted-death co-ordination teams.
What other steps has Ontario taken to support medical assistance in dying?
Ontario introduced Bill 84, the Medical Assistance in Dying Statute Law Amendment Act, 2016, to clarify several issues that fall within provincial jurisdiction. This includes amendments to:
- the Coroners Act and the Vital Statistics Act, mandating that the physician or nurse practitioner who provided the medical assistance in dying shall give notice of the death to a coroner, and clarifying that the Coroner does not need to sign the medical certificate of death for MAID deaths unless the Coroner investigates the death (see also our Issue Backgrounder #10, “Planned Deaths at Home”)
- the Excellent Care for All Act, clarifying that MAID may not be used as a reason to deny a payout on insurance or other benefits, and providing immunity from proceedings for damages to physicians, nurse practitioners, and any other persons assisting them in the lawful performance of MAID
- the Freedom of Information and Protection of Privacy Act and the Municipal Freedom of Information and Protection of Privacy Act, to protect the identities of clinicians and institutions that provide MAID from being disclosed pursuant to an FOI request
- the Workplace Safety and Insurance Act, ensuring that a claim made under the WSIA where the worker received MAID would be determined based on the illness or disease for which the worker was determined to be eligible to receive MAID and not another cause of death.
Where can I get more detailed information on this topic?
The LCO’s Improving the Last Stages of Life Discussion Paper (May 2017) discusses the law and practices around medical assistance in dying in greater depth. Specifically, see the discussion at chapter 3.C and 4.E.
What kinds of questions is the LCO asking?
Outside this scope of proposed legislation, the LCO has heard about several additional provincial-level issues related to MAID. These include questions related to:
- transitions between care settings to receive MAID (see our Issue Backgrounder #4, “Transitions Between Care”), and challenges in receiving MAID at home (see our Issue Backgrounder #10, “Planned Deaths at Home”)
- conscientious objection to the provision of MAID services in long-term care
- appeals of capacity determinations for persons requesting MAID, and
- policies and practices that could be put in place to preempt or resolve disputes arising from the above (see our Issue Backgrounder #5, “Resolving Health Care Disputes”).
The LCO is therefore interested in hearing your views:
- What strategies or law reform measures would effectively address the grief, bereavement, employment and support needs of caregivers and family members supporting someone in the last stages of dying?
How can I share my views on this issue?
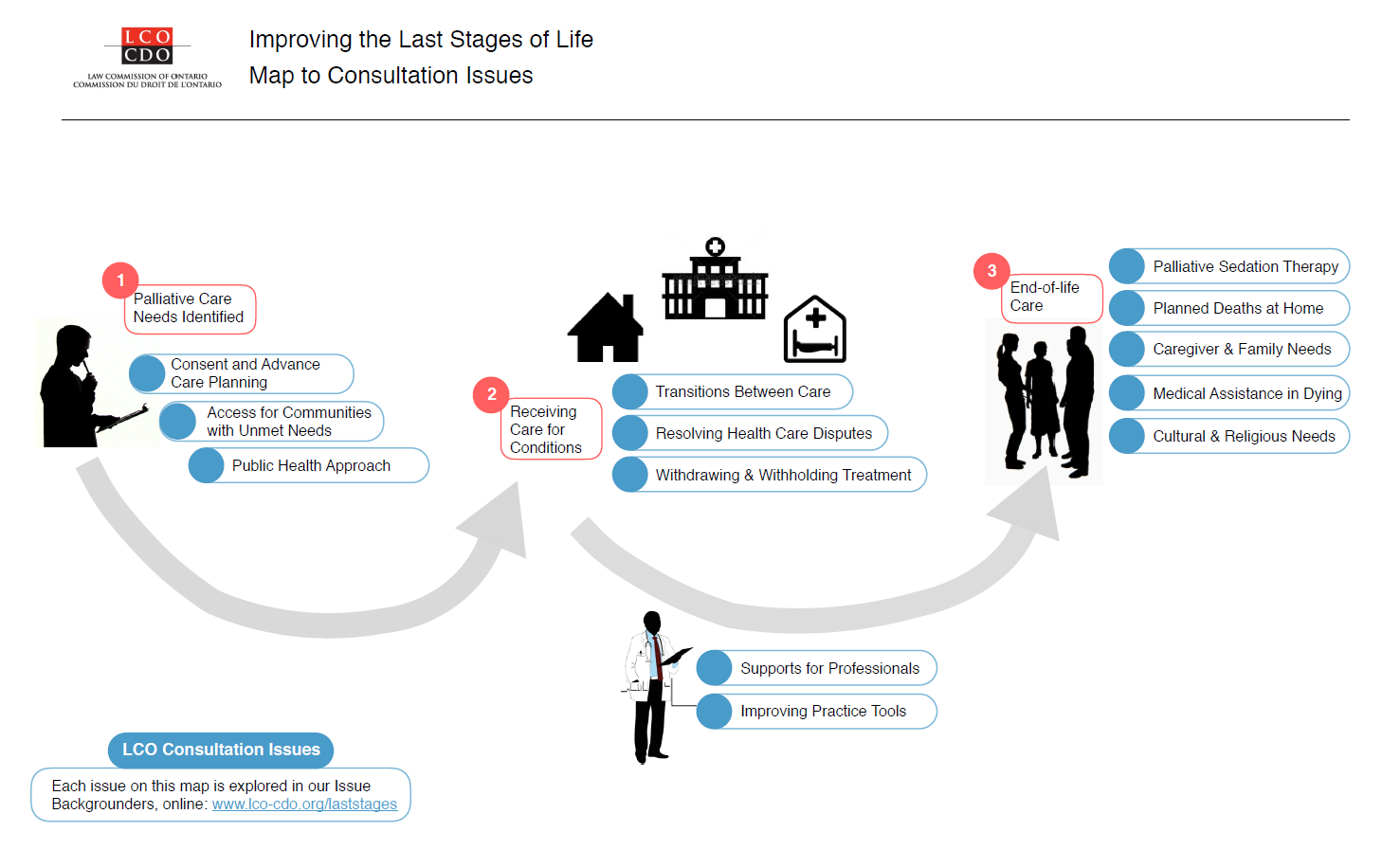
A fuller examination of these issues is available in our Executive Summary and Discussion Paper. We’ve also summarized other issues in a Consultation Issues Map and Issue Backgrounders.
{kind=link}
LCO’s formal consultation period runs from May – September 2017. The LCO invites your participation through:
- The project website at http://www.lco-cdo.org/laststages
- Written submissions at any time to lawcommission@lco-cdo.org
- Watch live and archived webcast consultation sessions
- Complete the consultation survey on your mobile, tablet, or computer
- Propose an in-person focus group for your community
- Contacting Project Research Lawyer Ryan Fritsch through the contact information below
Law Commission of Ontario Toronto (416) 650-8406
Project on Improving the Last Stages of Life Toll-Free (866) 950-8406
2032 Ignat Kaneff Building
Osgoode Hall Law School, York University Fax (416) 650-8418
4700 Keele Street, Toronto, ON M3J 1P3 E-mail: lawcommission@lco-cdo.org
Written submissions will be accepted until September 29, 2017