
What is the Last Stages of Life Project?
The Law Commission of Ontario (LCO) is Ontario’s leading law reform agency. The goal of our Improving the Last Stages of Life project is to identify and recommend law reforms in the “last stages of life.” This is a broad and inclusive term that allows us to look at rights and legal issues in end-of-life planning, palliative care, medical assistance in dying, and other issues. An important aspect of this is establishing a public health approach to palliative care, the subject of this backgrounder. This backgrounder is one of a series of consultation documents the LCO has developed for this project.
This document is a brief overview intended to raise issues and stimulate discussion for the purposes of LCO’s consultations. This document should not be relied on as a source of law.
What is the role of faith and cultural needs in the last stages of life?
Faith and culture are integral to attitudes about care nearing the end of life and perceptions of quality in health care services. While Ontario strives to improve equitable and high quality palliative care, it should consider strengthening services that reflect deeply held patient values and wishes for community engagement. As the Fraser Report explains, Ontarians have pronounced views “about the importance of ensuring that all patients have access to culturally appropriate and safe palliative and end-of-life care.”
The LCO has chosen to use the terms “faith” and “culture” for their broad scope and regular usage among stakeholders whom we consulted. We intended these terms to be inclusive of other words relevant to the issues the project reviews such as “religion”, “ethnicity”, “ancestry” and “language”. We also acknowledge they might overlap with additional social concepts such as “race.” We further acknowledge that the LCO cannot describe examples of beliefs and practices among Ontario’s diverse communities without being reductive.
How does faith and culture influence decisions in the last stages of life?
LCO’s discussion paper examines a wide array of cultural and faith practices, and commissioned research adds to this discussion. Below, we simply highlight general ways in which faith and culture influence care for the dying. Our purpose is to identify moments when heightened attention to faith and culture is due:
- Treatment decisions: Patients and SDMs may take faith and cultural beliefs into account when making decisions about life-sustaining treatments. Some belief systems are uncomfortable with mainstream health services; others maintain that life support should be provided indefinitely until a person dies. Between the two, there is a spectrum of beliefs about withholding and withdrawing life support, medical assistance in dying and the receipt of non-traditional treatment.
- Practices during illness: Faith and cultural communities may exercise meaningful practices during illness, such as prayer and ceremonies. Practices are expressive and may require adaptive physical environments that can accommodate singing and music, smoke, prostration and visitations from community members that may exceed standardized allowances, and impact on other patients too. Practices may occur at key junctures in the illness trajectory that could require adjustments to procedural routine.
- Significant community figures: Community figures may embody a sense of history and collective experience. For instance, elderly persons who survived past atrocities emanating from hate and discrimination can hold special significance for community members. Family and community members might expect these figures to receive particularly respectful treatment.
- Care for the deceased: Caring for the deceased may involve a variety of practices, ranging from prayer to tending to the body and burial ceremonies. There may be a critical order for the succession of practices. Community members may also request to be involved in physical after-death care, and to exclude health care providers. Keeping the deceased’s body “whole” is a central belief for many faiths and cultures, which organ donation or autopsies might offend.
The above description of moments when faith and culture are engaged during the dying process is admittedly limited. Other recurring themes that the LCO heard about include food preferences, language needs and continued contact with faith and cultural peers, especially in long-term care homes.
It is also important to recognize the distinct need for “cultural safety.” This term aims to recognize the interconnectedness of Indigenous health with the continuing repercussions of colonization, cultural and social assimilation and persisting systemic discrimination, which have led to trauma within communities and a loss of culture. Thus, cultural safety involves awareness about power imbalances between health care providers and Indigenous patients, the incorporation of Indigenous understandings of death and dying, healing practices, traditional foods, spirituality, and language and cultural translation as integral to the provision of quality care.
What is the legal framework for faith and cultural rights in the last stages of life?
Our discussion paper goes examines Canadian and provincial law protecting faith and cultural rights. This can include the Charter of Rights, the Human Rights Code, as well as other rights and principles relevant to ensuring equality and substantive justice in health care services. Further rights and principles that could apply to faith and cultural communities stem from the Ontario Human Rights Commission policy on creed, and Indigenous rights.
On the whole, these laws do not paint a cogent picture of what rights faith and cultural communities are entitled to on the ground. Faith and cultural rights are complicated by their connection with capacity and decision-making, and child protection laws.
Ontario’s health care system is also fragmented across sectors, meaning separate laws may contain various provisions relating to faith and cultural preferences. For instance, legislation governing long-term care homes establish rights to be placed in facilities and to receive services that respond to preferences based on ethnic, spiritual, religious, linguistic, familial and cultural factors. These rights are balanced by the fact that long-term care is a group living environment, and residents frequently share rooms. Similarly, tenants in retirement homes also have a right to have their “lifestyle and choices respected and to freely pursue [their] social, cultural, religious, spiritual and other interests.” However, as retirement homes are residential tenancies, these rights may not substantially interfere with the reasonable enjoyment of the home for the licensee and other residents.
What are some issues in supporting faith and cultural needs in practice?
The LCO commissioned a research study that offers insights into the adequacy of faith and cultural accommodations and supports in hospitals. Their findings demonstrate that there appears to be no uniform approach across the province to achieving faith and culturally sensitive care. Regulatory colleges and professional association provide guidance, but education for health care providers is variable.
Health care providers indicate they do not feel comfortable providing culturally competent and safe care because they receive little formal education to serve patients in this respect. Aside from the lack of education, they spoke about difficulties with requiring health care providers to take on added areas of competence, which could increase their workload.
Some said there should be a dedicated person with the expertise to address faith and cultural preferences in facilities. Currently in hospitals, there are few formal policies on faith and cultural issues. There is a common perception in Ontario that chaplaincy programs are not essential services, and they are the first to be cut when resources are low or system restructuring takes place.
Often, patients and families are not asked about their preferences at the bedside and are left to coordinate their own faith and cultural supports. They may not be aware of the available supports, or be in a position to advocate for them. If accommodations or supports are denied, pathways to enforcement are unclear.
Where can I get more detailed information on this topic?
The LCO’s Improving the Last Stages of Life Discussion Paper (May 2017) discusses the law and practices around faith and cultural needs in greater depth. Specifically, see the discussion at chapter 3.C, chapter 5, and chapter 6.G. See also the expert paper commissioned by the Law Commission for this project, “Integrating religious and cultural supports into quality care in the last stages of life in Ontario.”
What kinds of questions is the LCO asking?
There are multiple strategies that could be used to improve culturally competent and safe care in Ontario. Possible solutions that service providers and community members spoke to LCO about include creating educational tools for cultural competence and safety. The LCO could also review the possibilities for requiring Ontario’s regulatory institutions and care settings to create and implement formal policies on faith and cultural integration. Although the LCO’s understanding of faith and cultural competence and safety goes beyond accommodations, we would also like to know if more detailed guidance from the OHRC is warranted.
- What approaches are best suited to address barriers, accommodations and supports to better integrate faith, cultural and spiritual practices into care nearing the end of life?
How can I share my views on this issue?
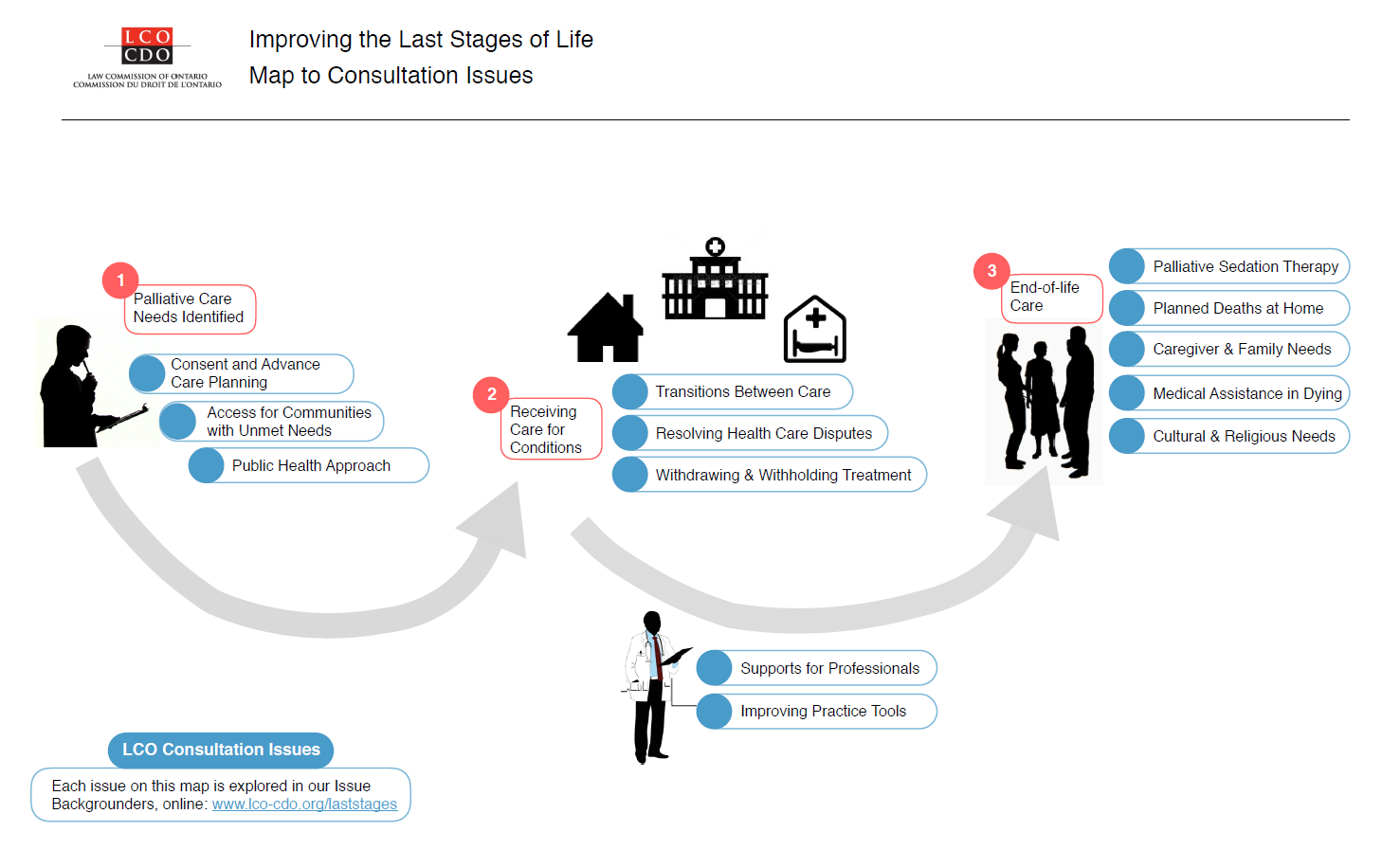
A fuller examination of these issues is available in our Executive Summary and Discussion Paper. We’ve also summarized other issues in a Consultation Issues Map and Issue Backgrounders.
{kind=link}
LCO’s formal consultation period runs from May – September 2017. The LCO invites your participation through:
- The project website at http://www.lco-cdo.org/laststages
- Written submissions at any time to lawcommission@lco-cdo.org
- Watch live and archived webcast consultation sessions
- Complete the consultation survey on your mobile, tablet, or computer
- Propose an in-person focus group for your community
- Contacting Project Research Lawyer Ryan Fritsch through the contact information below
Law Commission of Ontario Toronto (416) 650-8406
Project on Improving the Last Stages of Life Toll-Free (866) 950-8406
2032 Ignat Kaneff Building
Osgoode Hall Law School, York University Fax (416) 650-8418
4700 Keele Street, Toronto, ON M3J 1P3 E-mail: lawcommission@lco-cdo.org
Written submissions will be accepted until September 29, 2017