
What is the Last Stages of Life Project?
The Law Commission of Ontario (LCO) is Ontario’s leading law reform agency. The goal of our Improving the Last Stages of Life project is to identify and recommend law reforms in the “last stages of life.” This is a broad and inclusive term that allows us to look at rights and legal issues in end-of-life planning, palliative care, medical assistance in dying, and other issues. An important aspect of this is access for communities with unmet needs, the subject of this backgrounder. This backgrounder is one of a series of consultation documents the LCO has developed for this project.
This document is a brief overview intended to raise issues and stimulate discussion for the purposes of LCO’s consultations. This document should not be relied on as a source of law.
Why is it important to look at different communities in the last stages of life?
The issues raised in the LCO’s project affect all Ontarians because each of us dies and is affected by the deaths of those around us. But different communities have different traditions, values and expectations to the last stages of life, and thus different needs in terms of access, accommodation, information and outreach. LCO’s inclusive approach to defining care in the last stages of life means we must account for diversity in Ontario’s communities and regulatory frameworks.
We hope to learn more about these traditions, values and expectations in our consultations.
The LCO also wants to know about the views, perspectives, and values of the people and institutions who govern and implement these laws as professionals, health care agencies or institutions, government and delegated agencies. Our project strives to understand the difficulties they encounter in providing services and supports to persons who are directly affected.
Which communities are affected and what are their needs?
Recent government reviews of palliative care confirm that Ontarians suffer marked disparities in accessing quality care in the last stages of life. Changing demographics and social determinants of health such as age, disability, LGBTQ identity, Indigenous identity, income level, place of residence, mental health and culture can also strongly affect the setting, type and quality of care that Ontarians receive.
These are just a few examples of how different communities may have different needs in relation to the last stages of life:
- Different medical conditions. Persons with cancer receive the most publicly funded services for palliative care in Ontario (about 30%). But at least the same proportion of Canadians die from other categories of illnesses, including circulatory and respiratory diseases (about 29%). Multiple sclerosis, amyotrophic lateral sclerosis (ALS), and kidney disease are further examples of progressive illnesses that may affect fewer people, but could develop slowly, and should have access to high quality, personalized care.
- Ontarians living with HIV. The onset on HIV-associated neurocognitive disorders (HAND) is younger than those with Alzheimer’s disease. The disorder comes as a surprise for many and can trigger concerns for financial planning, the availability of HIV-designated services, and intersecting needs.
- Persons living with dementia. Among deaths due to chronic conditions in Canada, Alzheimer’s underwent the largest growth from 2000 to 2009 (growing about 25%). About 90% of persons diagnosed with dementia transition from living in the community to long-term care before their death. The important process of health care consent and advance care planning has thus been identified in our project as an important area of the law for this community of Ontarians to better ensure values, beliefs and wishes are made aware.
- At some point in life, most Ontarians act as a caregiver to a family member or friend. Up to 75% of care in Canada is provided voluntarily by unpaid individuals and 97% of patients receiving home care in Ontario get assistance from a caregiver. Caregivers told the LCO that the time and effort required by such daily tasks can be incredibly difficult to manage without supports (such as paid benefits and respite)
- Faith and cultural communities. Religion and culture strongly influence beliefs and practices surrounding death for individuals, families, health care providers and communities. Faith and cultural leaders have begun to address ethical approaches to the last stages of life in recent years with some having delivered positions on the appropriateness of different courses of treatment, or directly providing counsel, leading prayer, mediating disputes and performing rituals after death.
- First Nations, Inuit and Metis Communities. Indigenous peoples are affected by shorter life expectancy, higher rates of chronic conditions and distressing health crises. The palliative care that any one individual receives is highly dependent on factors such as status under the Indian Act, place of residence within or outside a First Nations jurisdiction, and the geographical location and resources of distinctive First Nation communities. There is greater need for health care providers to create culturally appropriate and locally designed and controlled palliative care programs.
- Homeless persons. Homelessness affects diverse individuals who are living in extremely vulnerable circumstances – from persons affected by family violence staying in shelters and immigrants in temporary accommodations to “unsheltered” persons living on the streets. Equitable and early access to effective palliative care can be a significant challenge for homeless and vulnerably housed patients. The LCO heard that homeless persons suffer considerable prejudice, which affects not only the quality of care they receive, but also has a chilling effect on their willingness to seek out help.
- Rural and remote communities. Diverse communities face unique barriers accessing palliative care, such as rural and northern communities, francophone persons, cultural groups and Indigenous peoples. Specific barriers to these goals that the LCO has heard about include the lack of long-term and palliative care on reserves and in rural and remote communities, and a lack of access to medical assistance in dying.
- Persons with disabilities. The heightened vulnerability of persons with disability who are nearing death is attributable to social factors including prejudice, marginalization, social isolation and substantial experiences of abuse and neglect. Vulnerabilities are especially felt by persons with diminished cognitive capacity, who may not know their options, or face challenges communicating their needs and concerns. Even where services are accessed, persons with disabilities can have complex care needs which limit the breadth of options available to them.
Where can I get more detailed information on this topic?
The LCO’s Improving the Last Stages of Life Discussion Paper (May 2017) offers a detailed discussion of the law and practices around providing access for communities with unmet needs. Specifically, see the discussion at chapter 2.C and chapter 5.
What kinds of questions is the LCO asking?
The LCO has made efforts to explore how diversity influences the issues under consideration in the project. We hope to learn more about these traditions, values and expectations in our consultations:
- Within the scope of LCO’s project, are there any additional affected individuals, communities, and institutions that should be taken into account?
- What has your experience been with the last stages of life as a member or ally of a community of need?
- What law reforms do you believe are needed for communities with unmet needs, and how would such reforms be most effectively implemented in law?
How can I share my views on this issue?
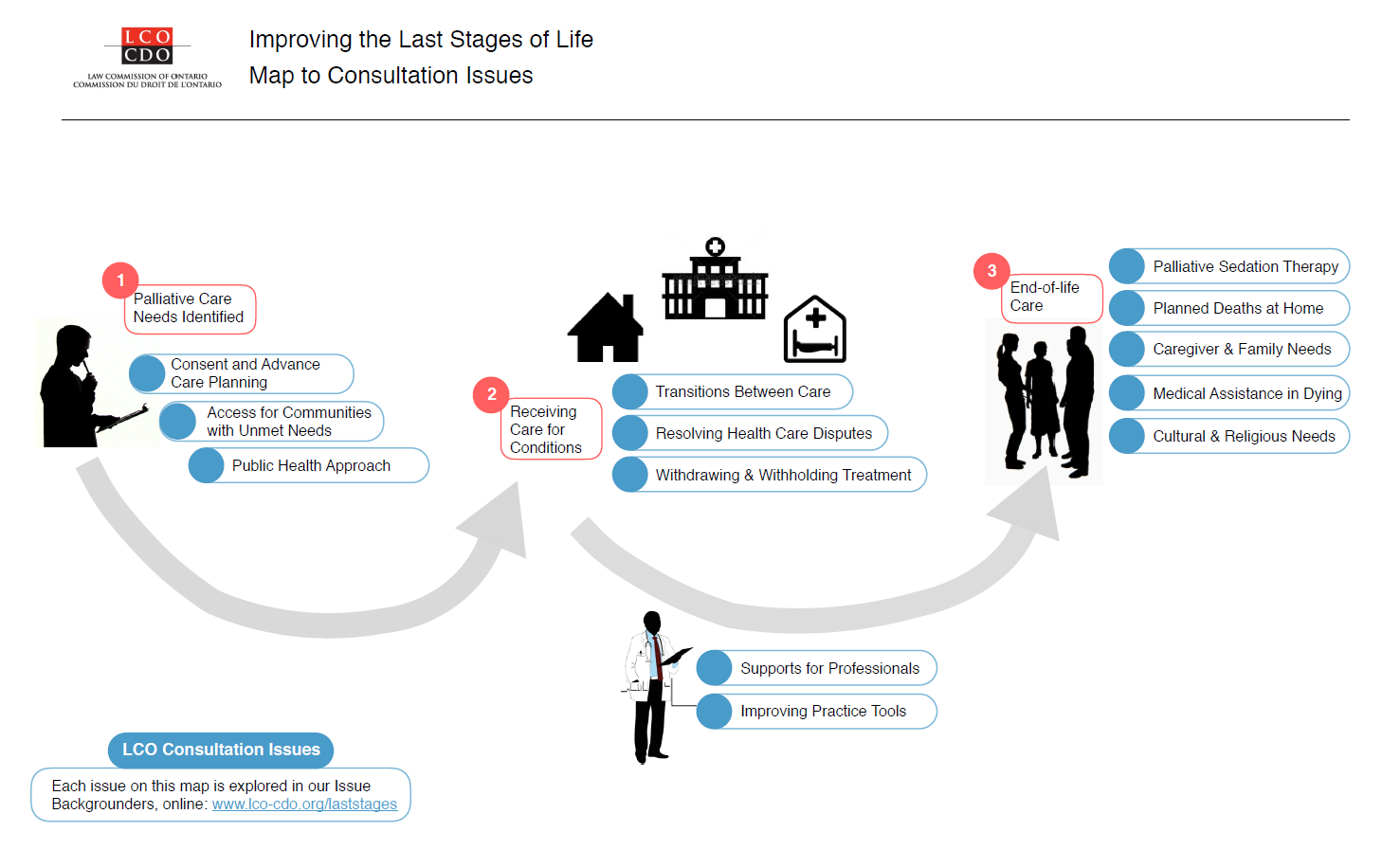
A fuller examination of these issues is available in our Executive Summary and Discussion Paper. We’ve also summarized other issues in a Consultation Issues Map and Issue Backgrounders.
{kind=link}
LCO’s formal consultation period runs from May – September 2017. The LCO invites your participation through:
- The project website at http://www.lco-cdo.org/laststages
- Written submissions at any time to lawcommission@lco-cdo.org
- Watch live and archived webcast consultation sessions
- Complete the consultation survey on your mobile, tablet, or computer
- Propose an in-person focus group for your community
- Contacting Project Research Lawyer Ryan Fritsch through the contact information below
Law Commission of Ontario Toronto (416) 650-8406
Project on Improving the Last Stages of Life Toll-Free (866) 950-8406
2032 Ignat Kaneff Building
Osgoode Hall Law School, York University Fax (416) 650-8418
4700 Keele Street, Toronto, ON M3J 1P3 E-mail: lawcommission@lco-cdo.org
Written submissions will be accepted until September 29, 2017