
What is the Last Stages of Life Project?
The Law Commission of Ontario (LCO) is Ontario’s leading law reform agency. The goal of our Improving the Last Stages of Life project is to identify and recommend law reforms in the “last stages of life.” This is a broad and inclusive term that allows us to look at rights and legal issues in end-of-life planning, palliative care, medical assistance in dying, and other issues. An important aspect of this is establishing a public health approach to palliative care, the subject of this backgrounder. This backgrounder is one of a series of consultation documents the LCO has developed for this project.
This document is a brief overview intended to raise issues and stimulate discussion for the purposes of LCO’s consultations. This document should not be relied on as a source of law.
What kinds of legal disputes arise in the last stages of life, and how are they addressed?
Death, dying and bereavement are highly emotional and important experiences for everyone involved – patients, family, friends and health care providers, alike.
Conflicts in the last stages of life may revolve around health care decision-making, eligibility for services or concerns about the quality of care being provided. Disagreements can take place in multiple care settings about many different matters. Disputes may involve patients, SDMs, family members, health care facility and providers. Some of the most common disputes within the context of the LSL include:
Disputes regarding Consent and Decision Making
Experience has demonstrated that there are many disputes regarding the provision of health care consent during the last stages of life. For example, health care providers and SDMs may disagree about whether life-sustaining procedures should be withheld or withdrawn.
Disputes of this kind can adjudicated by the Consent and Capacity Board (CCB). The CCB is an independent tribunal with jurisdiction over issues raised under Ontario’s Health Care Consent Act (HCCA). Different individuals can initiate the CCB review process depending on the type of application. For instance, a health care provider can apply to determine if a substitute decision maker (SDM) has complied with the rules for decision-making. Health care providers and SDMs can also apply to the CCB for directions about an incapable person’s treatment decisions. Many disputes may also resolve informally among those involved, without resort to the CCB, or where a facility offers their own dispute resolution mechanisms.
A study of CCB decisions concerning a patient’s best interests in end-of-life situations identified several themes, including where health care providers suggest that life-sustaining treatments be withdrawn where the SDM disagrees; and where SDMs rely on their own values and religious beliefs in their interpretations of best interest of the patient.
Disputes regarding eligibility for, and quality of, services and supports
When a member of the public believes they received substandard care, or were found ineligible for services and supports, there are several dispute mechanisms in place.
Regulatory colleges like the College of Physicians and Surgeons of Ontario or the College of Nurses of Ontario are required to maintain complaints procedures for members of the public who allege they received substandard care. If the complainant or health care provider wishes to dispute the resolution of such a complaint they can apply to the Health Professions Appeal and Review Board (HPARB). HPARB has powers to confirm the decision, refer the matter back, make recommendations, or require the committee to do things within its jurisdiction, such as requiring the health care provider to take remedial action.
Individuals applying for government-funded services that are administered at home or in the community may appeal a refusal to provide them with the level or type of services they requested to the Health Services Appeal and Review Board (HSARB).
Other existing dispute resolution mechanisms
In addition to these mechanisms, Ontario also has the following dispute resolution processes:
- Under the Excellent Care for All Act, 2010, hospitals are required to have a “patient relations process” to review complaints from patients and caregivers. Practices vary from hospital to hospital. These services may include access to patient advocates, medical ethicists, or involve legal counsel on behalf of the health team.
- Privately retained lawyers and other private patient advocacy services often represent patients and family members.
- Ontario has a number of medico-legal partnerships involving legal aid clinics or law student volunteers who attend at hospitals and other facilities to provide legal information and advice about a wide range of issues, though generally not in regards to patient advocacy within the health facility itself
- The Ontario government has established a Patient Ombudsman intended to “help meet the needs of patients who have not had their concerns resolved through existing complaint mechanisms” and covering public hospitals, long-term care homes and community care access corporations.
What are some issues with dispute resolution?
The LCO has heard a number of concerns regarding these processes. For example:
- Do Not Resuscitate orders. One of the areas of high dispute also occurs when health providers allegedly issue “Do-Not-Resuscitate” (DNR) orders without obtaining informed consent from a patient or SDM. As this issue could be dealt with as a matter of capacity and decision-making law, there appears to be some overlap in the cases that individuals bring to the CCB and the health boards (by way of the regulatory college complaints procedures).
- Cases relating to palliative and end-of-life care. HPARB in particular has heard a significant number of complaints related to delays in providing palliative care, failures to consult family members about transferring a patient to palliative care, discharges from hospital into the community, and failures to communicate the risks of harm associated with treatments. (See also Issue Backgrounder #4, “Transitions Between Care”).
- Access to early alternative dispute resolution (ADR) mechanisms. Stakeholders told us that the majority of disputes are actually resolved in a person’s care setting through good communication practices between health care providers, patients and SDMs. However, the LCO is aware that there are various critiques of internal resolution policies and processes. In these circumstances, earlier and expeditious access to ADR may be beneficial.
- Minimizing the causes of disputes. The LCO also heard that disagreements could be minimized by getting to their source, such as clarifying the law surrounding the withdrawal and withholding of treatment (see Issue Backgrounder #6, “Withdrawing and Withholding Treatment”) and providing accommodation and supports for faith and cultural communities (see Issue Backgrounder #13, “Cultural and Religious Needs”).
- Awareness of resolution mechanisms. More generally, patients and their families usually have only limited understanding of the available dispute resolution processes, and so may not access them or may not use them effectively. On the other hand, many health care providers expressed reluctance to use CCB processes. These professionals viewed the process as inappropriately adversarial, time-consuming, and in some cases, as not aligned with their values and their understanding of their roles.
Where can I get more detailed information on this topic?
The LCO’s Improving the Last Stages of Life Discussion Paper (May 2017) discusses the law and practices around dispute resolution in greater depth. Specifically, see the discussion at chapter 4.F and chapter 7.C. Please also see the findings and recommendations made in the LCO’s recently completed Legal Capacity, Guardianship and Decision-Making Final Report (March 2017) at chapter 7, “Rights Enforcement and Dispute Resolution: Empowering Individuals.”
What kinds of questions is the LCO asking?
The LCO’s project is considering a number of related questions about how to improve dispute resolution processes in the last stages of life:
- What strategies, processes or institutions are best suited to quickly or even pre-emptively resolving disputes nearing the end of life?
- How can legal information or education about dispute resolution mechanisms and frameworks be made more relevant, timely and effective in the last stages of life?
- Are there issues that would benefit from greater legal clarity and preempt disputes?
- What kinds of dispute resolution mechanisms do you think are accessible and effective?
How can I share my views on this issue?
A fuller examination of these issues is available in our Executive Summary and Discussion Paper. We’ve also summarized other issues in a Consultation Issues Map and Issue Backgrounders.
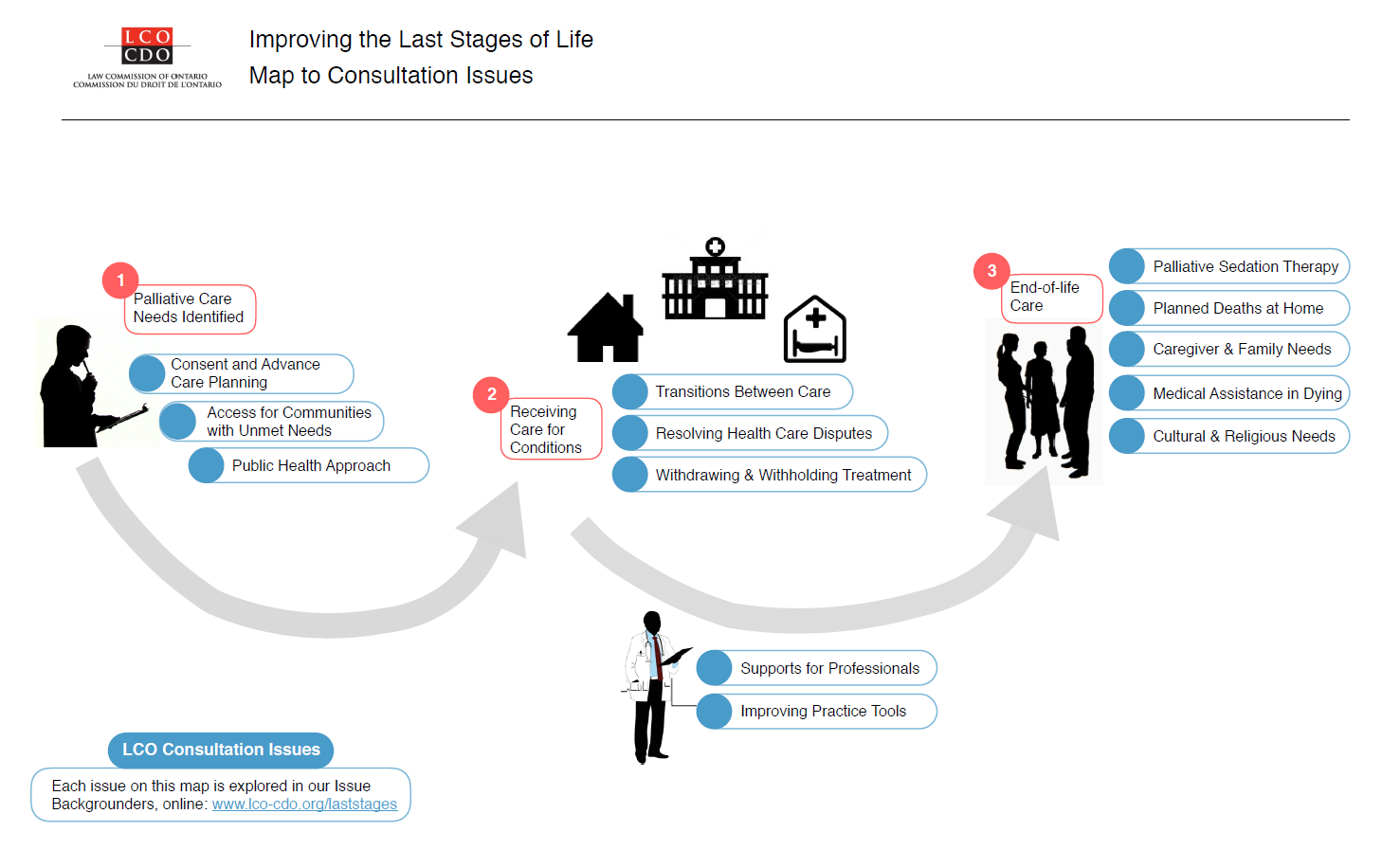{kind=link}
LCO’s formal consultation period runs from May – September 2017. The LCO invites your participation through:
- The project website at http://www.lco-cdo.org/laststages
- Written submissions at any time to lawcommission@lco-cdo.org
- Watch live and archived webcast consultation sessions
- Complete the consultation survey on your mobile, tablet, or computer
- Propose an in-person focus group for your community
- Contacting Project Research Lawyer Ryan Fritsch through the contact information below
Law Commission of Ontario Toronto (416) 650-8406
Project on Improving the Last Stages of Life Toll-Free (866) 950-8406
2032 Ignat Kaneff Building
Osgoode Hall Law School, York University Fax (416) 650-8418
4700 Keele Street, Toronto, ON M3J 1P3 E-mail: lawcommission@lco-cdo.org
Written submissions will be accepted until September 29, 2017