
What is the Last Stages of Life Project?
The Law Commission of Ontario (LCO) is Ontario’s leading law reform agency. The goal of our Improving the Last Stages of Life project is to identify and recommend law reforms in the “last stages of life.” This is a broad and inclusive term that allows us to look at rights and legal issues in end-of-life planning, palliative care, medical assistance in dying, and other issues. An important aspect of this is establishing a public health approach to palliative care, the subject of this backgrounder. This backgrounder is one of a series of consultation documents the LCO has developed for this project.
This document is a brief overview intended to raise issues and stimulate discussion for the purposes of LCO’s consultations. This document should not be relied on as a source of law.
What is the role of withdrawing and withholding treatment in the last stages of life?
Many Ontarians have personal experience making decisions about life-sustaining practices from our own health conditions or those of our family and friends. Some of these questions are about whether to withhold lifesaving treatment (i.e., CPR) when the situation appears hopeless, or to withdraw life-sustaining treatment (i.e., life support) when there is little or no chance of recovery. Aside from medical treatment, assistance with eating and drinking also becomes increasingly vital nearing the end of life. These are important – but subtle – distinctions in medical care and practise. Each has different implications in law and policy about who has authority to make decisions, and when.
What kinds of principles, rights or values influence these situations?
Decision-making in these situations is extremely difficult; it relies on confronting and defining our values and emotions. Decision-making in these situations also raises complex issues about the relationship between medical and legal ethics, principles and rights. For example, health care providers may view their role as only providing what they see as clinically beneficial treatment. By way of contrast, patients or family members may believe that they should have the right to request treatments above and beyond those that are clinically beneficial. Patients, family and health care providers may also disagree about what constitutes a “benefit.” As a result, decision-making regarding withdrawing or withholding treatments raise important medical and legal questions regarding:
- autonomy and self-determination
- beneficience (the ethical and professional obligations of a health care provider to alleviate suffering and provide treatment that benefits the patient)
- non-maleficence (to refrain from providing treatment that would harm the patient)
- utility (refraining from offering or continuing a treatment that is useless or ineffective)
- distributive justice (given that no health system has unlimited resources to provide all that is medically possible to everyone), and
- the value of life (its intrinsic value in religious, ethical and legal frameworks)
What questions arise in these situations?
In Canada, it is legal for capable persons to refuse life-sustaining and lifesaving treatment and for their substitute decision makers to do so on behalf of a person who is incapable.
The law is also clear that individuals (or SDMs) have the right to refuse life-sustaining treatment. And further, that consent must be obtained to withdraw treatment from a person who is already being treated.
However, the law is less clear – or at least unsettled – as to whether providers can legally withhold treatment by simply not proposing it to the patient or SDM from the outset if they believe it would not benefit the patient in the first place. Nor is the law clear if and when patients (or SDMs) can insist on treatment when health care providers do not agree.
The lack of clarity in the law has very important practical consequences. For example, there are many debates on whether health care providers have authority to not offer CPR, or if CPR can only be withheld on consent, or if CPR can be insisted upon by an SDM where it has not been proposed. Similarly, there appear to be outstanding questions regarding decision-making authority to place “do not resuscitate” orders on patient’s charts.
Further issues arise regarding the powers exercised by SDMs
Ontario law specifies that SDMs must consider the patient’s prior capable wishes, values and beliefs, if known and applicable. If not, then to consider other factors, including whether treatment is likely to improve the person’s condition or well-being and prevent deterioration, and whether the benefits outweigh the risk of harm. Ontario’s Health Care Consent Act does not, however, provide guidance on how these diverse factors should be balanced. The best interests test under the HCCA can result in different outcomes depending on the patient’s wishes, values and beliefs, and medical condition.
Moreover, many health care providers told the LCO that the best interests test does not sufficiently address the principles of beneficence and non-malfeasance, and that they should have greater authority to make unilateral decisions about life-sustaining treatment. Health care providers also object to the prospect that they may be required by law to provide treatment they believe contravenes their professional and ethical responsibilities.
Other jurisdictions have taken various approaches. Australian legislation requires consent to place a DNR order, but also allow the withholding of CPR in “acute emergencies” under certain conditions. The UK legislates that physicians are generally entitled to determine the appropriateness of life-sustaining treatment, however, only a tribunal may permit both the withdrawal and withholding of life-sustaining treatment for patients in a permanent vegetative or minimally conscious state.
What about the necessities of eating and drinking?
There appear to be conflicting laws in Ontario respecting whether SDMs can refuse consent to the provision of food and water. This could, in turn, affect whether individuals can realize their own prior expressed wishes to die in this manner. If SDMs cannot refuse consent to the provision of food and water, there could be potential inconsistencies with laws that do permit them to refuse or withdraw consent to treatment, such as life support.
Could providing food and water be defined as “treatment” under the HCCA to clarify that consent from a person (or SDM) is required in these situations? Or, could legislation governing long-term care and home care be amended to clearly and expressly exclude SDMs from refusing to consent to the provision of food and water?
Where can I get more detailed information on this topic?
The LCO’s Improving the Last Stages of Life Discussion Paper (May 2017) discusses the law and practices around withdrawing and withholding treatment and other life-sustaining practices. Specifically, see the discussion at chapter 6.C, “Decision-Making Authority over Life-Sustaining Practices.”
What kinds of questions is the LCO asking?
Taking into account experiences in other jurisdictions and Ontario’s particular context, the LCO would like to know whether our current mix of approaches achieves the best possible balance for Ontarians.
- There are connecting laws, principles and policies regarding decision making for life-sustaining practices such as CPR, DN, and nutrition. What are the strengths, weaknesses and gaps in Ontario’s current legal framework for decision-making authority over life-sustaining practices?
- Who should have authority to determine whether life-sustaining and lifesaving treatment (e.g., CPR, DNR) is offered to, or withdrawn from, a patient – the patient (or SDM) or a health care provider? Under what circumstances?
- Should Ontario regulate the offering of food and water to persons nearing the end of life, including the authority of SDMs to consent to withholding necessities of life?
How can I share my views on this issue?
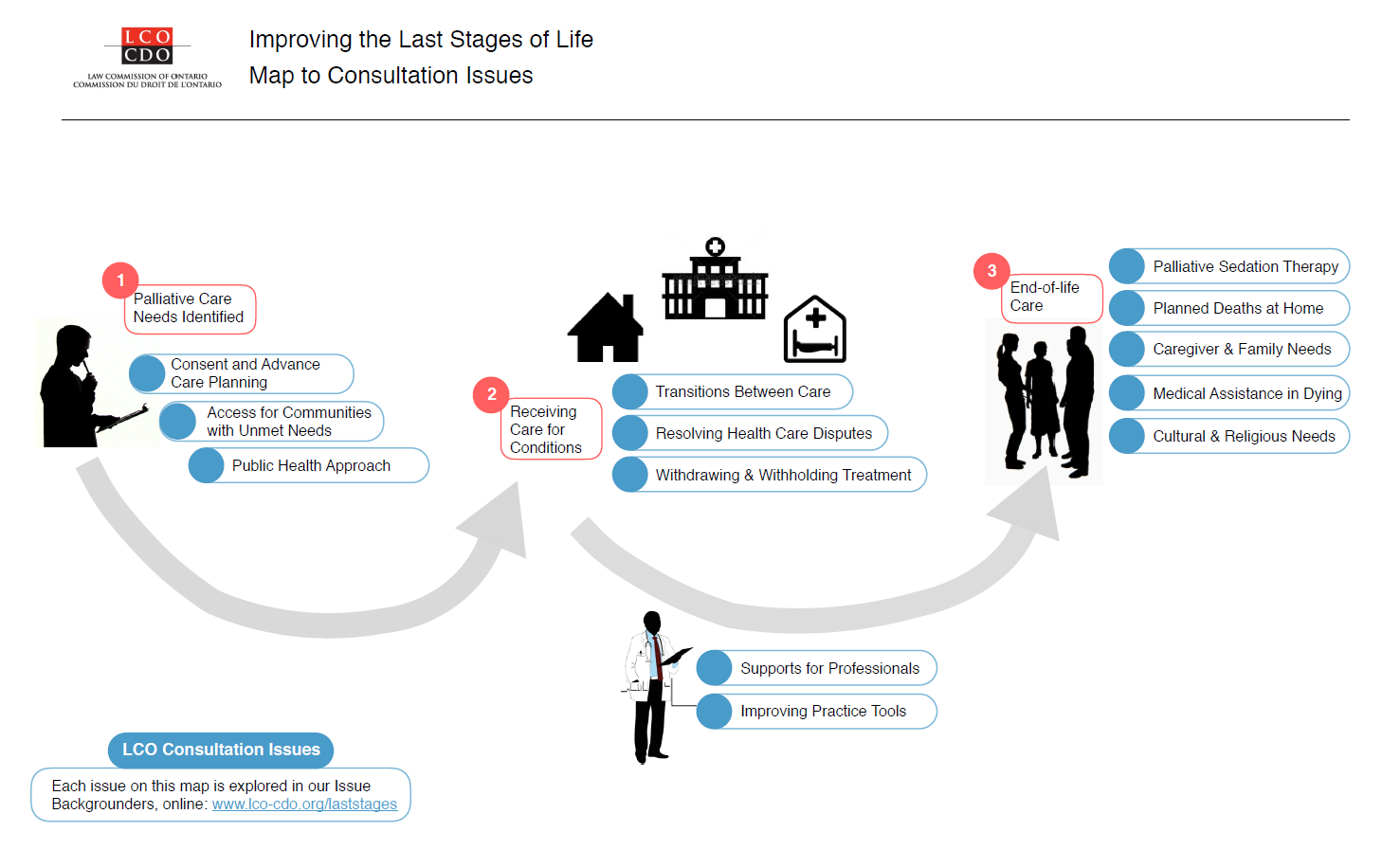
A fuller examination of these issues is available in our Executive Summary and Discussion Paper. We’ve also summarized other issues in a Consultation Issues Map and Issue Backgrounders.
{kind=link}
LCO’s formal consultation period runs from May – September 2017. The LCO invites your participation through:
- The project website at http://www.lco-cdo.org/laststages
- Written submissions at any time to lawcommission@lco-cdo.org
- Watch live and archived webcast consultation sessions
- Complete the consultation survey on your mobile, tablet, or computer
- Propose an in-person focus group for your community
- Contacting Project Research Lawyer Ryan Fritsch through the contact information below
Law Commission of Ontario Toronto (416) 650-8406
Project on Improving the Last Stages of Life Toll-Free (866) 950-8406
2032 Ignat Kaneff Building TTY (416) 650-8082
Osgoode Hall Law School, York University Fax (416) 650-8418
4700 Keele Street, Toronto, ON M3J 1P3 E-mail: lawcommission@lco-cdo.org
Written submissions will be accepted until September 29, 2017