
What is the Last Stages of Life Project?
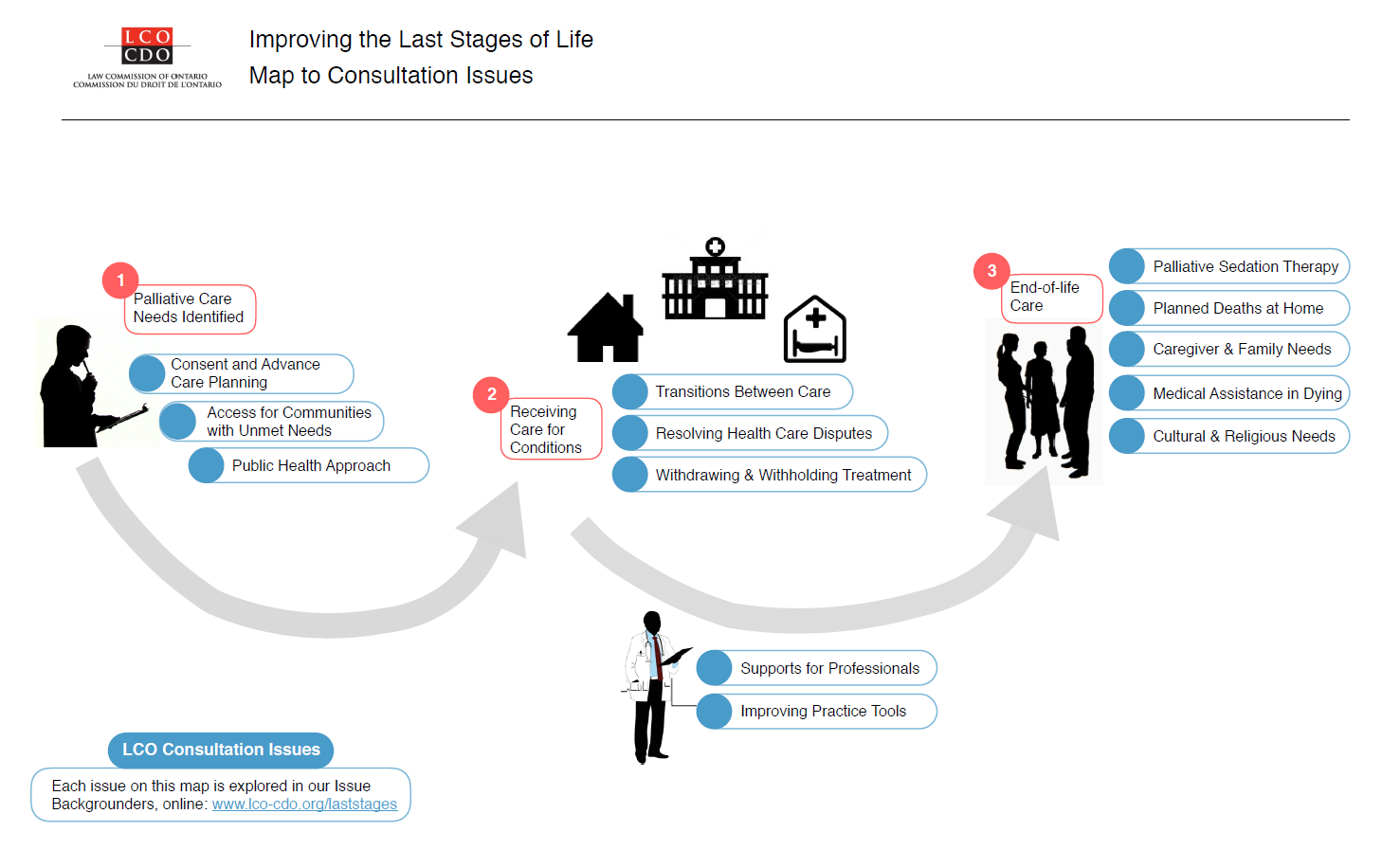
The Law Commission of Ontario (LCO) is Ontario’s leading law reform agency. The goal of our Improving the Last Stages of Life project is to identify and recommend law reforms in the “last stages of life.” This is a broad and inclusive term that allows us to look at rights and legal issues in end-of-life planning, palliative care, medical assistance in dying, and other issues. An important aspect of this is establishing a public health approach to palliative care, the subject of this backgrounder. This backgrounder is one of a series of consultation documents the LCO has developed for this project.
This document is a brief overview intended to raise issues and stimulate discussion for the purposes of LCO’s consultations. This document should not be relied on as a source of law.
What is palliative sedation therapy?
Palliative sedation therapy is an end-of-life treatment that is clinically and legally accepted in Canada. Palliative sedation therapy is intended to address the needs of patients who experience intolerable suffering from “refractory symptoms” that cannot be controlled by any tolerable therapy other than medications that reduce consciousness. The object of this therapy is not sedation itself, but symptom relief.
Palliative sedation therapy is intended to be a proportional response to symptoms, meaning that the level of sedation and duration vary. There are two main forms of palliative sedation:
- Continuous palliative sedation, which involves providing therapy until a person dies as a result of the natural course of illness, usually in the last hours or days of life.
- Respite sedation, which involves an agreement with the patient about a timeframe for sedation (e.g., 24 to 48 hours), after which the patient is awakened to determine if he or she would benefit from further therapy.
What are some of the issues that arise with palliative sedation therapy?
Palliative sedation therapy raises significant ethical concerns, especially when it is provided continuously. Generally speaking, this treatment engages similar principles to those arising in the context of other end-of-life practices, including beneficence, non-malfeasance, autonomy, self-determination and security (for more on those matters see Issue Backgrounder #6, “Withdrawing and Withholding Treatment”). Ethical concerns also arise with palliative sedation therapy for certain symptoms, such as psychological suffering. Most guidelines and policies do not recommend that psychological symptoms be considered sufficient for intervention, except in rare cases.
Proportionality is also a core principle for palliative sedation therapy. Proportionality comes into play when assessing whether palliative sedation should be used from the outset when there are less-invasive interventions that could be effective, and that doses should not be higher than needed to relieve suffering.
Another ethical concern that engages all of the principles listed above is that palliative sedation not be used to hasten death. Although palliative sedation may be provided until the point of death and may sometimes involve the withdrawal of life supports, from an ethical standpoint, it is not intended to hasten death, is thus ethically distinct from the practice of intentional killing. Nonetheless, there is a complex relationship between palliative sedation and medical assistance in dying. The LCO has heard that some patients, family and friends do seek to use palliative sedation as a form of medical assistance in dying.
What is the legal framework for palliative sedation therapy?
Palliative sedation is not currently the subject of a specific or separate regulatory regime in Ontario. And unlike the withdrawal and withholding of treatment and medical assistance in dying, palliative sedation has not been subject to a constitutional or other legal challenge. In the latter case, there are heightened safeguards against abuse, including the requirements for a second opinion, documented request, signatory witnesses and the presence of mental capacity up until the person receives treatment.
In terms of consent and decision-making, the Health Care Consent Act, 1996 applies to palliative sedation just as it does to other treatment decisions nearing the end of life, and thus requires informed consent from the patient or their substitute decision maker.
In Ontario, various regions and organizations have adopted policies and guidelines to regulate the practice, including the Canadian Society of Palliative Care Physicians, the College of Physicians and Surgeons of Ontario, and the Registered Nurses Association of Ontario. Other jurisdictions, like Quebec, have established a statutory framework for requesting and documenting palliative sedation therapy. This stipulates what must be provided for consent to be “informed”, and requires a request from a patient or SDM to be documented in a prescribed form and filed in the patient’s record.
The LCO has heard that this lack of an overarching framework can lead to complications, like a lack of consistency in operational definitions, a lack of documentation and recording of consent in patient records, limited safeguards to address vulnerabilities, and inconsistent use of terminology.
Where can I get more detailed information on this topic?
The LCO’s Improving the Last Stages of Life Discussion Paper (May 2017) discusses the law and practices around palliative sedation therapy in greater depth. Specifically, see the discussion at chapter 6.D. See also the related matters discussed in Issue Backgrounder #6, “Withdrawing and Withholding Treatment”
What kinds of questions is the LCO asking?
There are multiple avenues to improve clarity, consistency, safety and other challenges with palliative sedation therapy. Options for reform might include the following:
- creating a legislative framework to formalize the provision of palliative sedation with procedural protections that could describe requesting and documenting palliative sedation therapy, stipulating what must be provided for consent to be “informed”, and requiring documentation in a prescribed form. How would this consider existing laws around informed consent and medical assistance in dying?
- elaborating clinical guidelines through a taskforce or network approach (e.g., with the involvement of the Ontario Palliative Care Network or Ministry of Health and Long-term Care)
- requesting that regulatory colleges adopt thorough clinical guidelines.
How can I share my views on this issue?
A fuller examination of these issues is available in our Executive Summary and Discussion Paper. We’ve also summarized other issues in a Consultation Issues Map and Issue Backgrounders.
{kind=link}
LCO’s formal consultation period runs from May – September 2017. The LCO invites your participation through:
- The project website at http://www.lco-cdo.org/laststages
- Written submissions at any time to lawcommission@lco-cdo.org
- Watch live and archived webcast consultation sessions
- Complete the consultation survey on your mobile, tablet, or computer
- Propose an in-person focus group for your community
- Contacting Project Research Lawyer Ryan Fritsch through the contact information below
Law Commission of Ontario Toronto (416) 650-8406
Project on Improving the Last Stages of Life Toll-Free (866) 950-8406
2032 Ignat Kaneff Building
Osgoode Hall Law School, York University Fax (416) 650-8418
4700 Keele Street, Toronto, ON M3J 1P3 E-mail: lawcommission@lco-cdo.org
Written submissions will be accepted until September 29, 2017
[/fusion_text][/fusion_builder_column][/fusion_builder_row][/fusion_builder_container]